

Reduction of malaria transmission to Anopheles mosquitoes with a six-dose regimen of co-artemether
- PMID: 15839740
- PMCID: PMC1087200
- DOI: 10.1371/journal.pmed.0020092
Reduction of malaria transmission to Anopheles mosquitoes with a six-dose regimen of co-artemether
Abstract
Background: Resistance of malaria parasites to chloroquine (CQ) and sulphadoxine-pyrimethamine (SP) is increasing in prevalence in Africa. Combination therapy can both improve treatment and provide important public health benefits if it curbs the spread of parasites harbouring resistance genes. Thus, drug combinations must be identified which minimise gametocyte emergence in treated cases, and so prevent selective transmission of parasites resistant to any of the partner drugs.
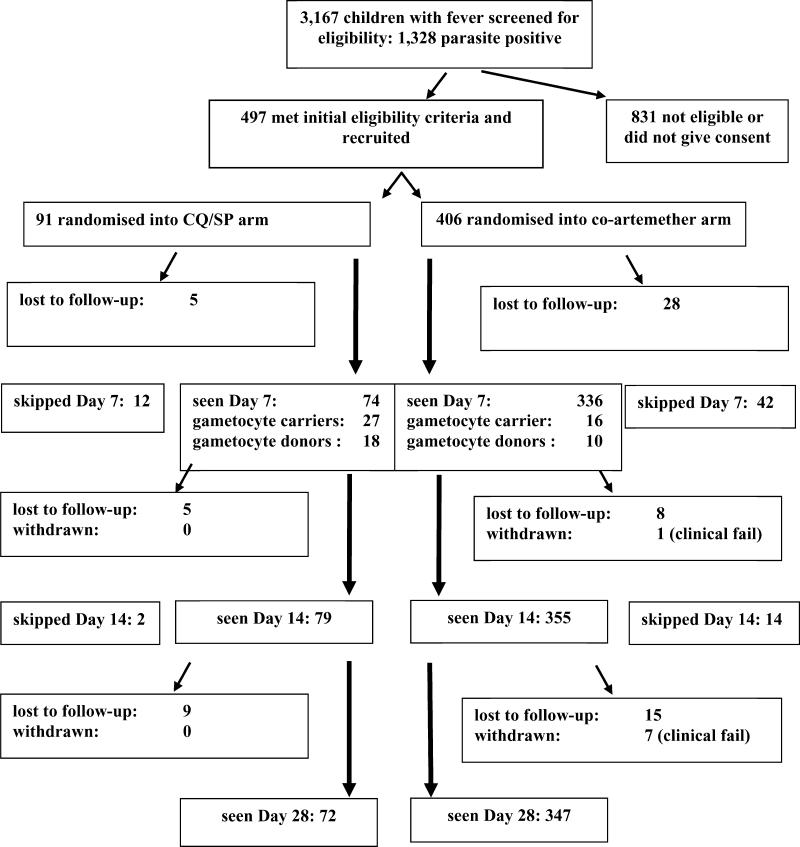
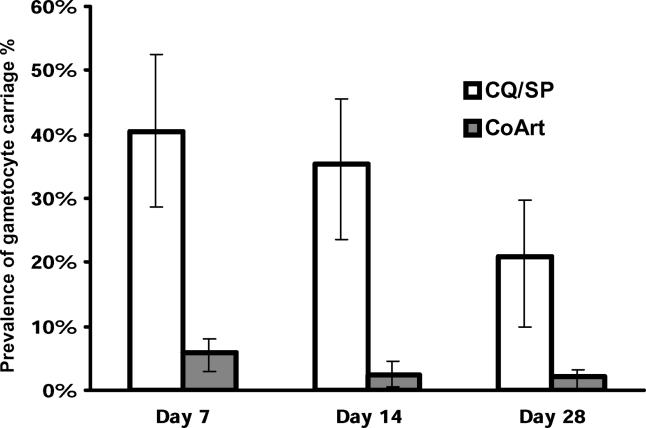
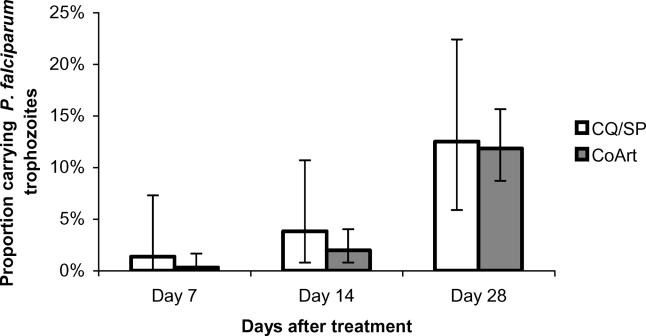
Methods and findings: In a randomised controlled trial, 497 children with uncomplicated falciparum malaria were treated with CQ and SP (three doses and one dose respectively; n = 91), or six doses of artemether in fixed combination with lumefantrine (co-artemether [Coartem, Riamet]) (n = 406). Carriage rates of Plasmodium falciparum gametocytes and trophozoites were measured 7, 14, and 28 d after treatment. The infectiousness of venous blood from 29 children carrying P. falciparum gametocytes 7 d after treatment was tested by membrane-feeding of Anopheles mosquitoes. Children treated with co-artemether were significantly less likely to carry gametocytes within the 4 weeks following treatment than those receiving CQ/SP (30 of 378 [7.94%] versus 42 of 86 [48.8%]; p < 0.0001). Carriers in the co-artemether group harboured gametocytes at significantly lower densities, for shorter periods (0.3 d versus 4.2 d; p < 0.0001) and were less infectious to mosquitoes at day 7 (p < 0.001) than carriers who had received CQ/SP.
Conclusions: Co-artemether is highly effective at preventing post-treatment transmission of P. falciparum. Our results suggest that co-artemether has specific activity against immature sequestered gametocytes, and has the capacity to minimise transmission of drug-resistant parasites.
Conflict of interest statement
Figures
References
-
- East African Network for Monitoring Antimalarial Treatment (EANMAT) The efficacy of antimalarial monotherapies, sulphadoxine-pyrimethamine and amodiaquine in East Africa: Implications for sub-regional policy. Trop Med Int Health. 2003;10:860–867. - PubMed
-
- Olliaro P, Mussano P. The Cochrane Library, Issue 4. Chichester, UK: John Wiley and Sons; 2003. Amodiaquine for treating malaria (Cochrane Re-view)
-
- Schellenberg D, Kahigwa E, Drakeley C, Malende A, Wigayi J, et al. The safety and efficacy of sulfadoxine-pyrimethamine, amodiaquine, and their combination in the treatment of uncomplicated Plasmodium falciparum malaria. Am J Trop Med Hyg. 67:17–23. - PubMed
-
- White NJ, Nosten F, Looareesuwan S, Watkins WM, Marsh K, et al. Averting a malaria disaster. Lancet. 1999;353:1965–1967. - PubMed
-
- Price R, Nosten F, Luxemburger C, Kuile FOT, Paiphun L, et al. Effects of artemisinin derivatives on malaria transmissibility. Lancet. 1996;347:1654–1658. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
