

ECG repolarization waves: their genesis and clinical implications
- PMID: 15842434
- PMCID: PMC6931934
- DOI: 10.1111/j.1542-474X.2005.05588.x
ECG repolarization waves: their genesis and clinical implications
Abstract
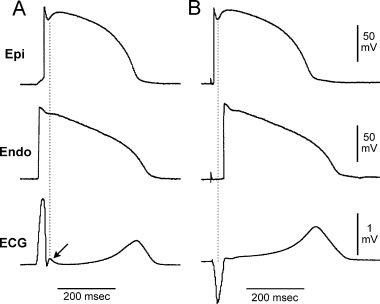
The electrocardiographic (ECG) manifestation of ventricular repolarization includes J (Osborn), T, and U waves. On the basis of biophysical principles of ECG recording, any wave on the body surface ECG represents a coincident voltage gradient generated by cellular electrical activity within the heart. The J wave is a deflection with a dome that appears on the ECG after the QRS complex. A transmural voltage gradient during initial ventricular repolarization, which results from the presence of a prominent action potential notch mediated by the transient outward potassium current (I(to)) in epicardium but not endocardium, is responsible for the registration of the J wave on the ECG. Clinical entities that are associated with J waves (the J-wave syndrome) include the early repolarization syndrome, the Brugada syndrome and idiopathic ventricular fibrillation related to a prominent J wave in the inferior leads. The T wave marks the final phase of ventricular repolarization and is a symbol of transmural dispersion of repolarization (TDR) in the ventricles. An excessively prolonged QT interval with enhanced TDR predisposes people to develop torsade de pointes. The malignant "R-on-T" phenomenon, i.e., an extrasystole that originates on the preceding T wave, is due to transmural propagation of phase 2 reentry or phase 2 early afterdepolarization. A pathological "U" wave as seen with hypokalemia is the consequence of electrical interaction among ventricular myocardial layers at action potential phase 3 of which repolarization slows. A physiological U wave is thought to be due to delayed repolarization of the Purkinje system.
Figures





References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
