

Olanzapine IM or velotab for acutely disturbed/agitated people with suspected serious mental illnesses
- PMID: 15846678
- PMCID: PMC6769079
- DOI: 10.1002/14651858.CD003729.pub2
Olanzapine IM or velotab for acutely disturbed/agitated people with suspected serious mental illnesses
Abstract
Background: People presenting with agitated or violent behaviour thought to be due to severe mental illness may require urgent pharmacological tranquillisation. Several preparations of olanzapine, an antipsychotic drug, are now being used for management of such agitation.
Objectives: To estimate the effects of intramuscular, oral-velotab, or standard oral olanzapine compared with other treatments for controlling aggressive behaviour or agitation thought to be due to severe mental illness.
Search strategy: We searched the Cochrane Controlled Trials Register (Issue 1, 2002), The Cochrane Schizophrenia Group's Register (November 2004) and reference lists. We contacted authors of trials and the manufacturers of olanzapine.
Selection criteria: Randomised clinical trials comparing oral-velotab or intramuscular, or standard oral olanzapine to any treatment, for agitated or aggressive people with severe mental illnesses.
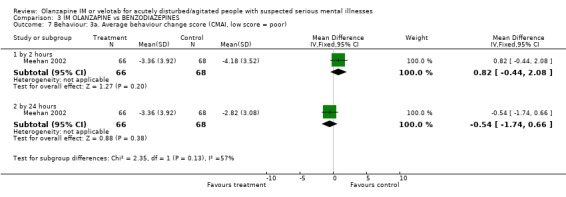
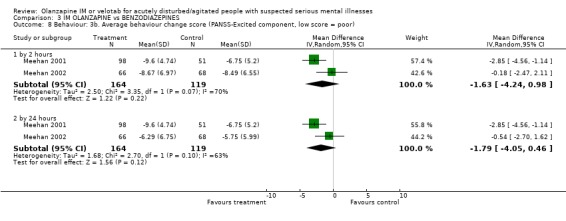
Data collection and analysis: We reliably selected, quality assessed and data extracted studies. For binary outcomes we calculated a fixed effects Risk Ratio (RR) and its 95% Confidence Interval (CI) with a weighted Number Needed to Treat/Harm statistic (NNT/H). For continuous outcomes, we preferred endpoint data to change data and synthesised non-skewed data from valid scales using a weighted mean difference (WMD).
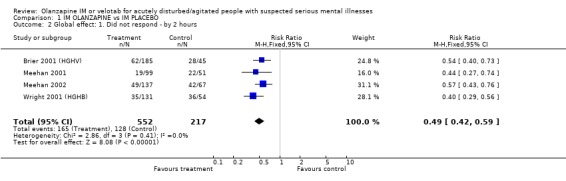
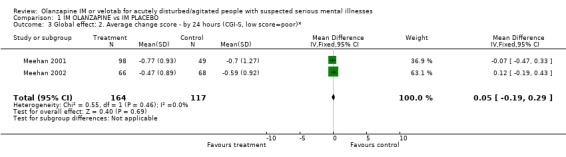
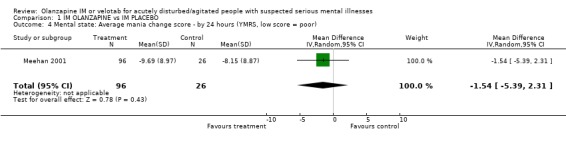
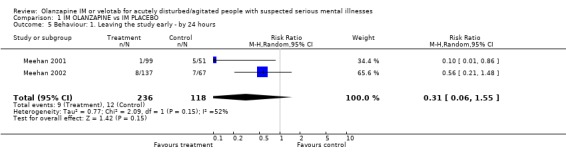
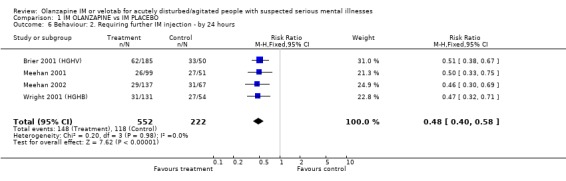
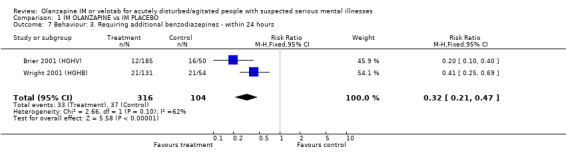
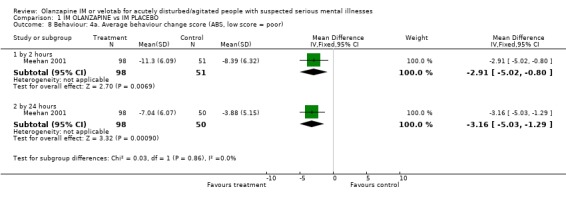
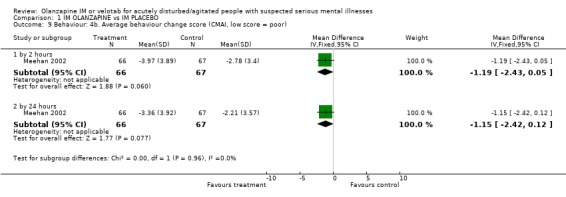
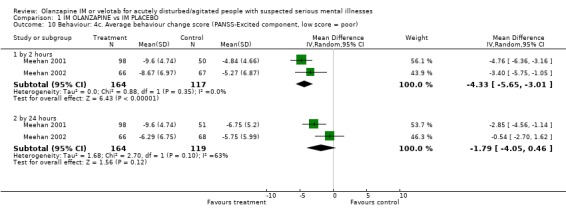
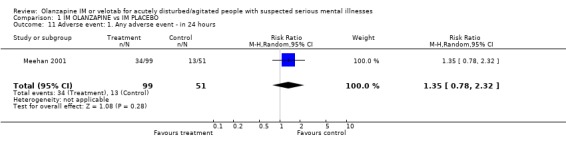
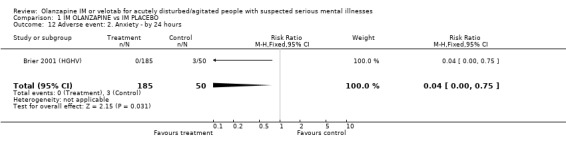
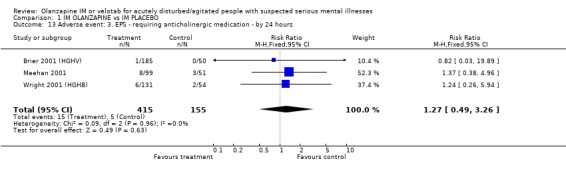
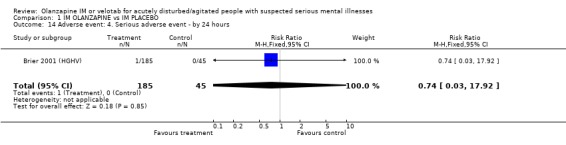
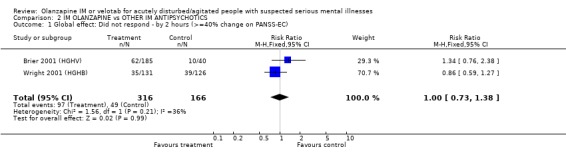
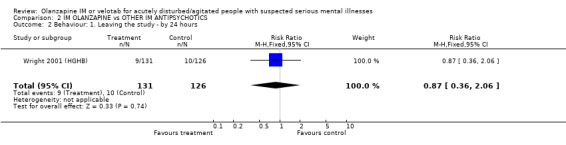
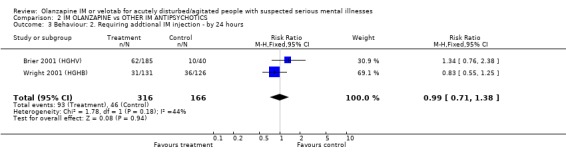
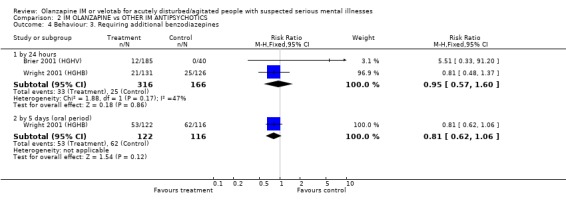
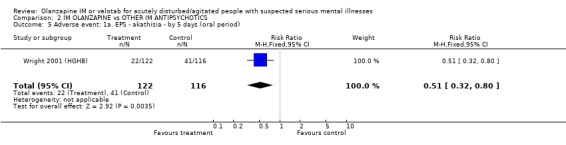
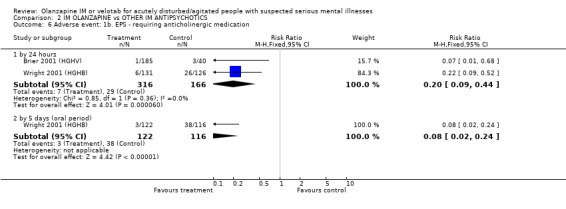
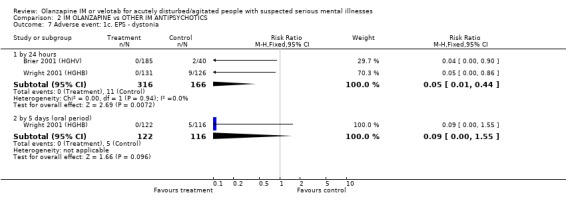
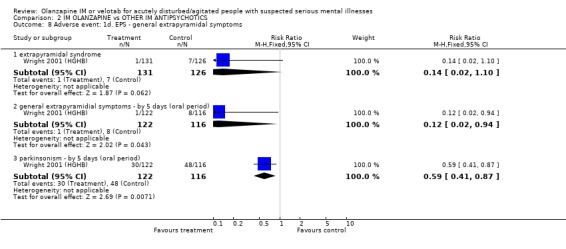
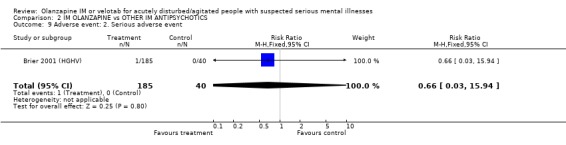
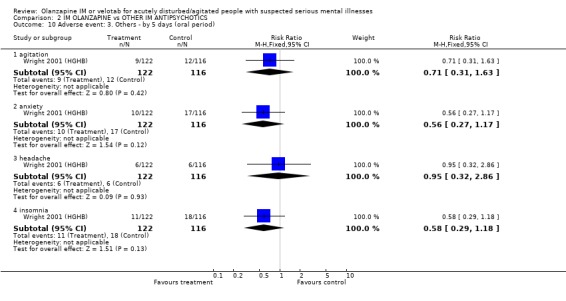
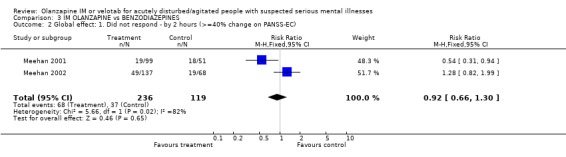
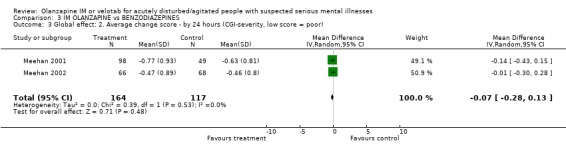
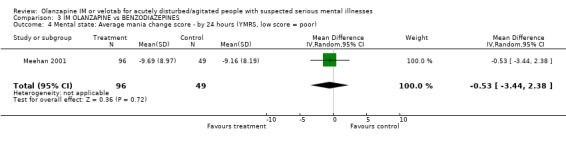
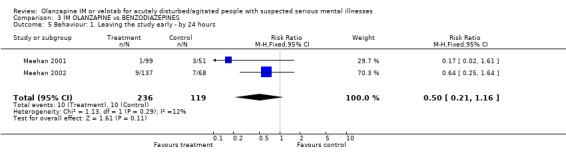
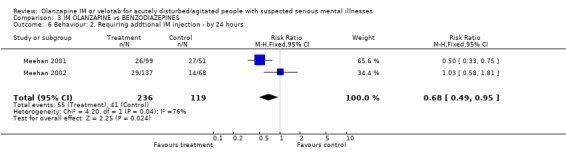
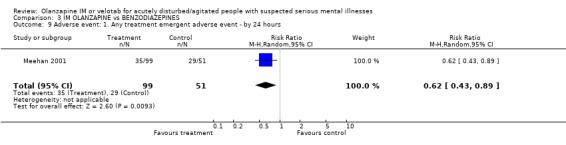
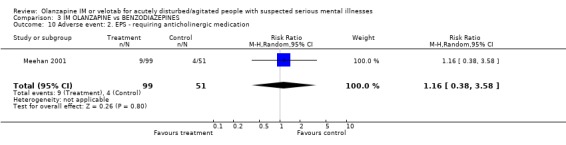
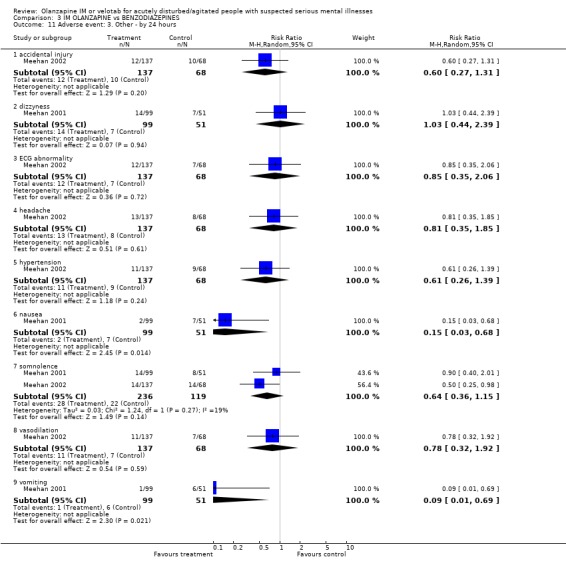
Main results: Four trials compared olanzapine IM with IM placebo (total n=769, 217 allocated to placebo). Fewer people given olanzapine IM had 'no important response' by 2 hours compared with placebo (4 RCTs, n=769, RR 0.49 CI 0.42 to 0.59, NNT 4 CI 3 to 5) and olanzapine IM was as acceptable as placebo (2 RCTs, n=354, RR leaving the study early 0.31 CI 0.06 to 1.55). When compared with placebo, people given olanzapine IM required substantially fewer additional injections following the initial dose (4 RCTs, n=774, RR 0.48 CI 0.40 to 0.58, NNT 4 CI 4 to 5). Olanzapine IM did not seem associated with extrapyramidal effects (4 RCT, n=570, RR experiencing any adverse event requiring anticholinergic medication in first 24 hours 1.27 CI 0.49 to 3.26). Two trials compared olanzapine IM with haloperidol IM (total n=482, 166 allocated to haloperidol). Studies found no differences between olanzapine IM and haloperidol by 2 hours for the outcome of 'no important clinical response' (2 RCTs, n= 482, RR 1.00 CI 0.73 to 1.38) neither was there a difference for needing repeat IM injections (2 RCTs, n=482, RR 0.99 CI 0.71 to 1.38). More people on haloperidol experienced akathisia over the five day oral period compared with olanzapine IM (1 RCT, n=257, RR 0.51 CI 0.32 to 0.80, NNT 6 CI 5 to 15) and fewer people allocated to olanzapine IM required anticholinergic medication by 24 hours compared with those given haloperidol IM (2 RCTs, n= 432, RR 0.20 CI 0.09 to 0.44, NNT 8 CI 7 to 11). Two trials compared olanzapine IM with lorazepam IM (total n=355, 119 allocated to lorazepam). For the outcome of 'no important clinical response' , there was no difference between people given olanzapine IM and those allocated to lorazepam at 2 hours (2 RCTs, n=355, RR 92 CI 0.66 to 1.30) but fewer people allocated to olanzapine IM required additional injections by 24 hours compared with those on lorazepam IM (2 RCTs, n=355, RR 0.68 CI 0.49 to 0.95, NNT 10 CI 6 to 59). People receiving IM olanzapine were less likely to experience any treatment emergent adverse events, than those on lorazepam (1 RCT, n=150, RR at 24 hours 0.62 CI 0.43 to 0.89, NNT 5 CI 4 to 17) and over the same time period there were no clear differences in the use of anticholinergic medication between groups (1 RCT, n=150, RR 1.16 CI 0.38 to 3.58).No studies reported outcomes related to hospital and service use. Nor did any report on issues of satisfaction with care or suicide, self-harm or harm to others. No studies evaluated the oro-dispersable form of olanzapine.
Authors' conclusions: Data relevant to the effects of olanzapine IM are taken from some studies that may not be considered ethical in many places, all are funded by a company with a pecuniary interest in the result. These studies often poorly report outcomes that are difficult to interpret for routine care. Other important outcomes are not recorded at all. Nevertheless, olanzapine IM probably has some value in helping manage acute aggression or agitation, especially where it is necessary to avoid some of the older, better, known treatments. Olanzapine causes fewer movement disorders than haloperidol and more than lorazepam. The value of the oro-dipersable velotab preparation is untested in trials. There is a need for well designed, conducted and reported randomised studies in this area. Such studies are possible and, we argue, should be designed with the patient groups and clinicians in mind. They should report outcomes of relevance to the management of people at this difficult point in their illness.
Conflict of interest statement
Mark Fenton ‐ has led Janssen, Lilly and Zeneca sponsored workshops for clinicians.
Ravindra Belgamwar ‐ none.
Figures
Update of
- doi: 10.1002/14651858.CD003729
References
References to studies included in this review
-
- Breier AF, Wright P, Birkett M, Meehan K, David SR, Brook S. Intramuscular olanzapine: dose‐related improvement in acutely agitated patients with schizophrenia. Annual Meeting of the American Psychiatric Association; 2001 May 5‐10; LA, USA. Marathon Multimedia, 2001. [MEDLINE: ; PMID 11431240]
-
- Meehan K, Zhang F, David S, Tohen M, Janicak P, Small J, Koch M, Rizk R, Walker D, Tran P, Breier A. A double‐blind, randomized comparison of the efficacy and safety of intramuscular injections of olanzapine, lorazepam, or placebo in treating acutely agitated patients diagnosed with bipolar mania.[see comment]. Journal of Clinical Psychopharmacology 2001;21(4):389‐97. [PMID 11476123] - PubMed
-
- Meehan KM, Wang H, David SR, Nisivoccia JR, Jones B, Beasley CM Jr, Feldman PD, Mintzer JE, Beckett LM, Breier A. Comparison of rapidly acting intramuscular olanzapine, lorazepam, and placebo: a double‐blind, randomized study in acutely agitated patients with dementia. Neuropsychopharmacology 2002;26(4):494‐504. [PMID 11927174] - PubMed
-
- Wright P, Birkett M, David SR, Meehan K, Ferchland I, Alaka KJ, Saunders JC, Krueger J, Bradley P, San L, Bernardo M, Reinstein M, Breier A. Double‐blind, placebo‐controlled comparison of intramuscular olanzapine and intramuscular haloperidol in the treatment of acute agitation in schizophrenia. American Journal of Psychiatry 2001;158(7):1149‐51. [MEDLINE: ; PMID 11431240] - PubMed
References to studies excluded from this review
-
- Bergstrom R, Mitchell M, Jewell H, Richards J, McEwan J, Hatcher B. Examination of the safety, tolerance, and pharmacokinetics of intramuscular (IM) olanzapine compared to oral olanzapine in healthy subjects. Schizophrenia Research. 1999; Vol. 1,2 & 3:305.
-
- Kinon BJ, Hill AL, Perehia DGS. Olanzapine orodispersible tablet in the treatment of acutely ill, non‐compliant schizophrenia patients. Journal of Psychopharmacology 2001;15(Suppl.3):1‐74.
-
- Wright P, Jewell H, Mitchell M, Hatcher B, Brook S, Kiesler G, Bergstrom G. A preliminary study of safety, efficacy, and pharmacokinetics of Intramuscular olanzapine in patients with non organic psychosis. Schizophrenia Research 1999;36(1,2, 3):318.
-
- Wright P, Keisler G, Mitchell M, Jewell H, Hatcher B, Brook S, Bergstrom R. Safety and efficacy of intramuscular olanzapinein patients with acute non organic psychosis. Schizophrenia Research 1999;36(1‐3):318.
Additional references
-
- Alexander J, Tharyan P, Adams CE, John T, Mol C, Philip J. Rapid tranquilisation of violent or agitated patients in a psychiatric emergency setting: a pragmatic randomised trial of intramuscular lorazepam versus haloperidol plus promethazine.. British Journal of Psychiatry 2004;185:63‐9. - PubMed
-
- Allen MH, Currier GW, Hughes DH, Reyes‐Harde M, Docherty JP, Expert Consensus Panel for Behavioral Emergencies. The Expert Consensus Guideline Series. Treatment of behavioral emergencies. Postgraduate Medicine 2001;May:1‐88. - PubMed
-
- Amdisen A, Nielsen MS, Dencker SJ, Fensbo C, Ahlfors UG, Gravem A, et al. Zuclopenthixol acetate in Viscoleo ‐ a new drug formulation. An open Nordic multicentre study of zuclopenthixol acetate in Viscoleo in patients with acute psychoses including mania and exacerbation of chronic psychoses. Acta Psychiatrica Scandinavia 1987;75:99‐107. - PubMed
-
- Barnes TR. A rating scale for drug‐induced akathisia. British Journal of Psychiatry 1989;154:672‐6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical