

Surgical management of hilar cholangiocarcinoma
- PMID: 15849505
- PMCID: PMC1357124
- DOI: 10.1097/01.sla.0000160701.38945.82
Surgical management of hilar cholangiocarcinoma
Abstract
Objective: To assess the surgical management of hilar cholangiocarcinoma over a time period when liver resection was considered standard management.
Summary background data: Hilar cholangiocarcinoma remains a difficult challenge for surgeons. An advance in surgical treatment is the addition of liver resection to the procedure. However, liver resection in the setting of liver dysfunction caused by biliary obstruction can be associated with increased mortality.
Methods: Between 1997 and 2004, 80 patients with hilar cholangiocarcinoma having surgery were reviewed. Fifty-three patients had attempted curative resections, 14 patients had palliative bypasses, while 13 patients had findings that precluded any further intervention. Twenty-three patients required portal vein resection and reconstruction to achieve negative margins, 3 of which also required reconstruction of the hepatic artery.
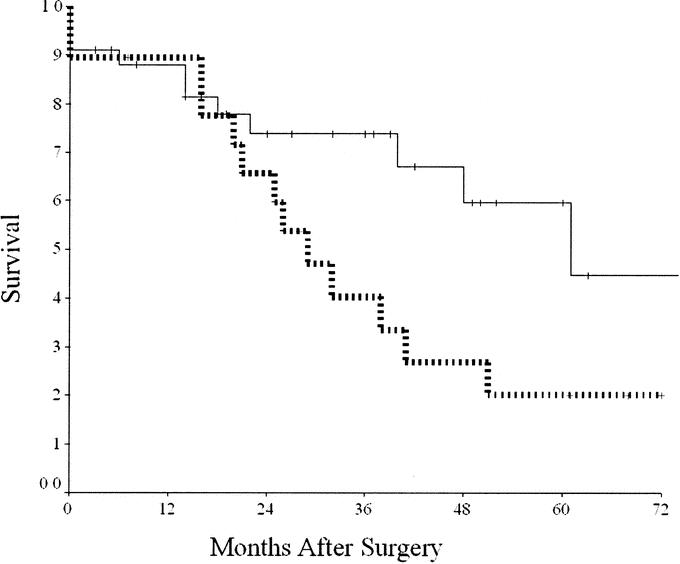
Results: Patients undergoing resection had a 9% operative mortality, with morbidity of 40%. Patients who demonstrated lobar hypertrophy preoperatively due to tumor involvement of the contralateral liver or induced with portal vein embolization (PVE) had a significantly lower operative mortality than those patients without hypertrophy. Median overall survival in patients resected was 40 months, with 5-year survival of 35%. Negative margins were achieved in 80% of cases and were associated with improved survival. Five-year survival in patients undergoing resection with negative margins was 45%.
Conclusion: Combined liver and bile-duct resection can be performed for hilar cholangiocarcinoma with acceptable mortality, though higher than that for liver resections performed for other indications. The use of PVE in cases where hypertrophy of the remnant liver has not occurred preoperatively may reduce the risk of operative mortality.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
