

Effect of surgical margin status on survival and site of recurrence after hepatic resection for colorectal metastases
- PMID: 15849507
- PMCID: PMC1357126
- DOI: 10.1097/01.sla.0000160703.75808.7d
Effect of surgical margin status on survival and site of recurrence after hepatic resection for colorectal metastases
Abstract
Objective: To evaluate the influence of surgical margin status on survival and site of recurrence in patients treated with hepatic resection for colorectal metastases.
Methods: Using a multicenter database, 557 patients who underwent hepatic resection for colorectal metastases were identified. Demographics, operative data, pathologic margin status, site of recurrence (margin, other intrahepatic site, extrahepatic), and long-term survival data were collected and analyzed.
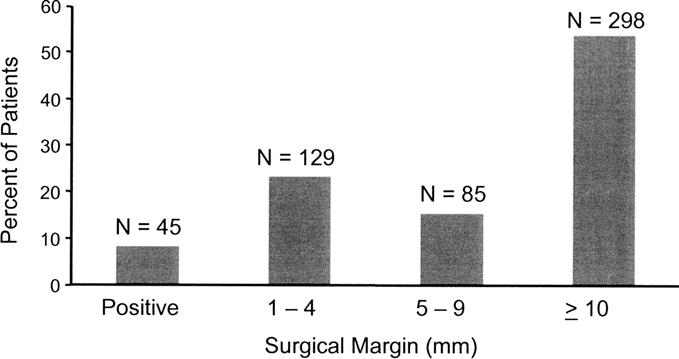
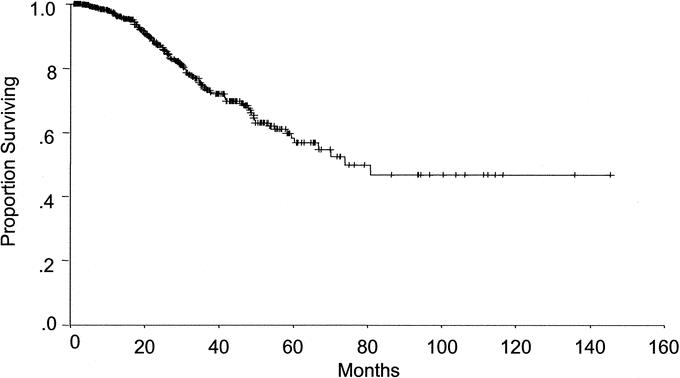
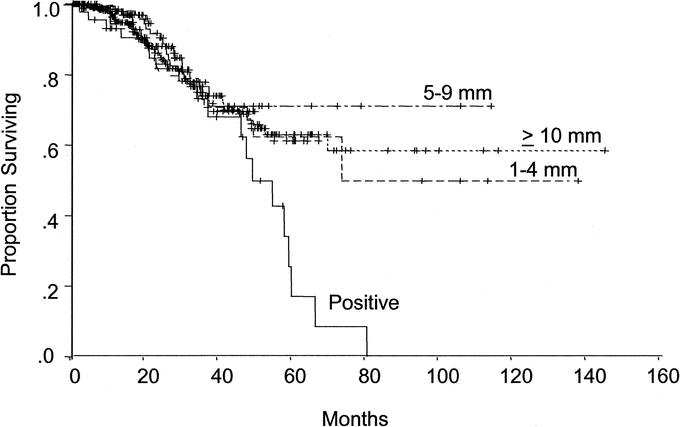
Results: On final pathologic analysis, margin status was positive in 45 patients, and negative by 1 to 4 mm in 129, 5 to 9 mm in 85, and > or =1 cm in 298. At a median follow-up of 29 months, the 1-, 3-, and 5-year actuarial survival rates were 97%, 74%, and 58%; median survival was 74 months. Tumor size > or =5 cm, >3 tumor nodules, and carcinoembryonic antigen level >200 ng/mL predicted poor survival (all P < 0.05). Median survival was 49 months in patients with positive margins and not yet reached in patients with negative margins (P = 0.01). After hepatic resection, 225 (40.4%) patients had recurrence: 21 at the surgical margin, 56 at another intrahepatic site, 82 at an extrahepatic site, and 66 at both intrahepatic and extrahepatic sites. Patients with negative margins of 1 to 4 mm, 5 to 9 mm, and > or =1 cm had similar overall recurrence rates (P > 0.05). Patients with positive margins were more likely to have surgical margin recurrence (P = 0.003). Adverse preoperative biologic factors including tumor number greater than 3 (P = 0.01) and a preoperative CEA level greater than 200 ng/mL (P = 0.04) were associated with an increased risk of positive surgical margin.
Conclusions: A positive margin after resection of hepatic colorectal metastases is associated with adverse biologic factors and increased risk of surgical-margin recurrence. The width of a negative surgical margin does not affect survival, recurrence risk, or site of recurrence. A predicted margin of <1 cm after resection of hepatic colorectal metastases should not be used as an exclusion criterion for resection.
Figures
Comment in
-
The study of cavitational ultrasonically aspirated material during surgery for colorectal liver metastases as a new concept in resection margin.Ann Surg. 2006 Oct;244(4):634-5. doi: 10.1097/01.sla.0000239631.74713.b5. Ann Surg. 2006. PMID: 16998378 Free PMC article. No abstract available.
References
-
- Scheele J, Stang R, Altendorf-Hofmann A, et al. Resection of colorectal liver metastases. World J Surg. 1995;19:59–71. - PubMed
-
- Adson MA, van Heerden JA, Adson MH, et al. Resection of hepatic metastases from colorectal cancer. Arch Surg. 1984;119:647–651. - PubMed
-
- Adam R, Avisar E, Ariche A, et al. Five-year survival following hepatic resection after neoadjuvant therapy for nonresectable colorectal. Ann Surg Oncol. 2001;8:347–353. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
