

Surgical management of bile duct injuries sustained during laparoscopic cholecystectomy: perioperative results in 200 patients
- PMID: 15849514
- PMCID: PMC1357133
- DOI: 10.1097/01.sla.0000161029.27410.71
Surgical management of bile duct injuries sustained during laparoscopic cholecystectomy: perioperative results in 200 patients
Abstract
Objective: A single institution retrospective analysis of 200 patients with major bile duct injuries was completed. Three patients died without surgery due to uncontrolled sepsis. One hundred seventy-five patients underwent surgical repair, with a 1.7% postoperative mortality and a complication rate of 42.9%.
Summary background data: The widespread application of laparoscopic cholecystectomy (LC) has led to a rise in the incidence of major bile duct injuries (BDI). Despite the frequency of these injuries and their complex management, the published literature contains few substantial reports regarding the perioperative management of BDI.
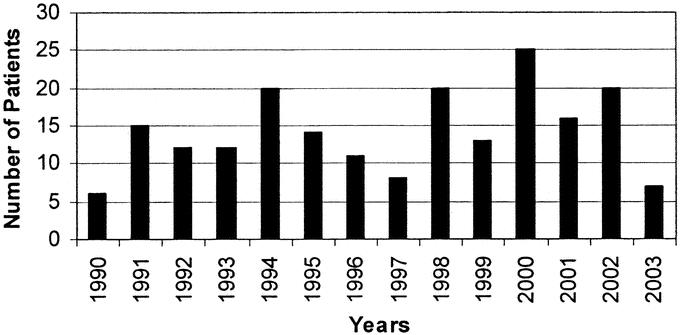
Methods: From January 1990 to April 2003, a prospective database of all patients with a BDI following LC was maintained. Patients' charts were retrospectively reviewed to analyze perioperative surgical management.
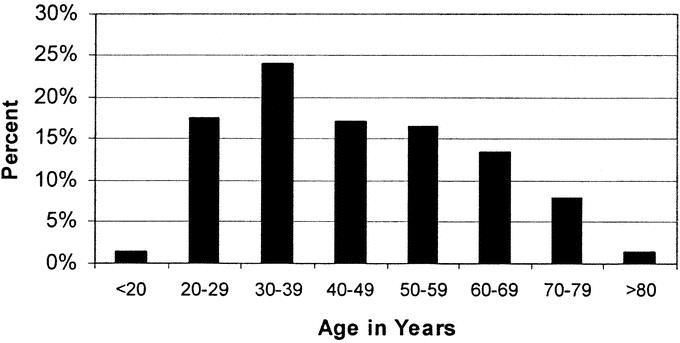
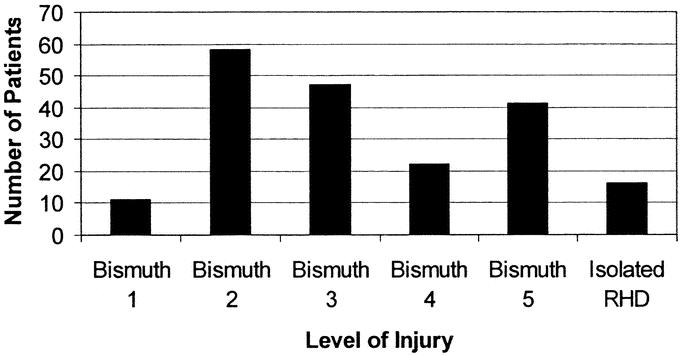
Results: Over 13 years, 200 patients were treated for a major BDI following LC. Patient demographics were notable for 150 women (75%) with a mean age of 45.5 years (median 44 years). One hundred eighty-eight sustained their BDI at an outside hospital. The mean interval from the time of BDI to referral was 29.1 weeks (median 3 weeks). One hundred nine patients (58%) were referred within 1 month of their injury for acute complications including bile leak, biloma, or jaundice. Twenty-five patients did not undergo a surgical repair at our institution. Three patients (1.5%) died after delayed referral before an attempt at repair due to uncontrolled sepsis. Twenty-two patients, having intact biliary-enteric continuity, underwent successful balloon dilatation of an anastomotic stricture. A total of 175 patients underwent definitive biliary reconstruction, including 172 hepaticojejunostomies (98%) and 3 end-to-end repairs. There were 3 deaths in the postoperative period (1.7%). Seventy-five patients (42.9%) sustained at least 1 postoperative complication. The most common complications were wound infection (8%), cholangitis (5.7%), and intraabdominal abscess/biloma (2.9%). Minor biliary stent complications occurred in 5.7% of patients. Early postoperative cholangiography revealed an anastomotic leak in 4.6% of patients and extravasation at the liver dome-stent exit site in 10.3% of patients. Postoperative interventions included percutaneous abscess drainage in 9 patients (5.1%) and new percutaneous transhepatic cholangiography and stent placement in 4 patients (2.3%). No patient required reoperation in the postoperative period. The mean postoperative length of stay was 9.5 days (median 9 days). The timing of operation (early, intermediate, delayed), presenting symptoms, and history of prior repair did not affect the incidence of the most common perioperative complications or length of postoperative hospital stay.
Conclusions: This series represents the largest single institution experience reporting the perioperative management of BDI following LC. Although perioperative complications are frequent, nearly all can be managed nonoperatively. Early referral to a tertiary care center with experienced hepatobiliary surgeons and skilled interventional radiologists would appear to be necessary to assure optimal results.
Figures
References
-
- Ko ST, Airan MC. Review of 300 consecutive laparoscopic cholecystectomies: development, evolution, and results. Surg Endosc. 1991;5:103–108. - PubMed
-
- Gadacz TR, Talamini MA, Lillemoe KD, et al. Laparoscopic cholecystectomy. Surg Clin North Am. 1990;70:1249–1262. - PubMed
-
- A prospective analysis of 1518 laparoscopic cholecystectomies: the Southern Surgeons Club. N Engl J Med. 1991;324:1073–1078. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
