

Perianal Crohn disease: predictors of need for permanent diversion
- PMID: 15849515
- PMCID: PMC1357134
- DOI: 10.1097/01.sla.0000161030.25860.c1
Perianal Crohn disease: predictors of need for permanent diversion
Abstract
Objective: Fissures, fistulas, abscesses, and anal canal stenosis are manifestations of perianal Crohn disease (CD). There are no known predictors of which patients will fail sphincter-sparing surgical therapy and ultimately require fecal diversion.
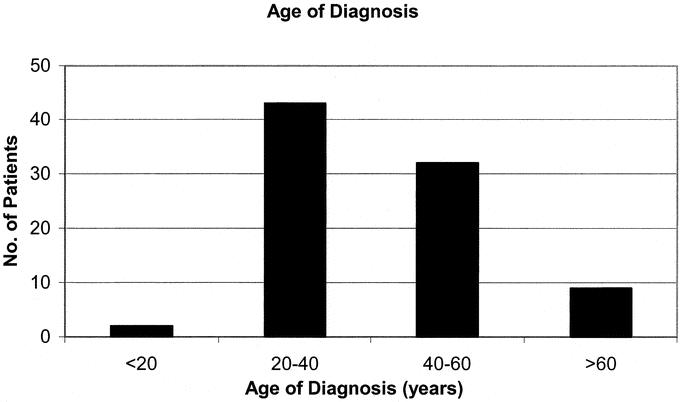
Methods: Of 356 consecutive patients with CD, 24% (86) had perianal CD (age range, 14-83 years), and women were slightly more frequently affected. Clinical variables were examined for factors predictive of the need for permanent fecal diversion.
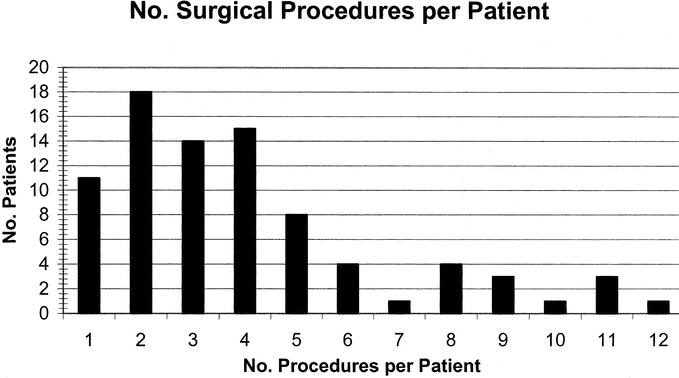
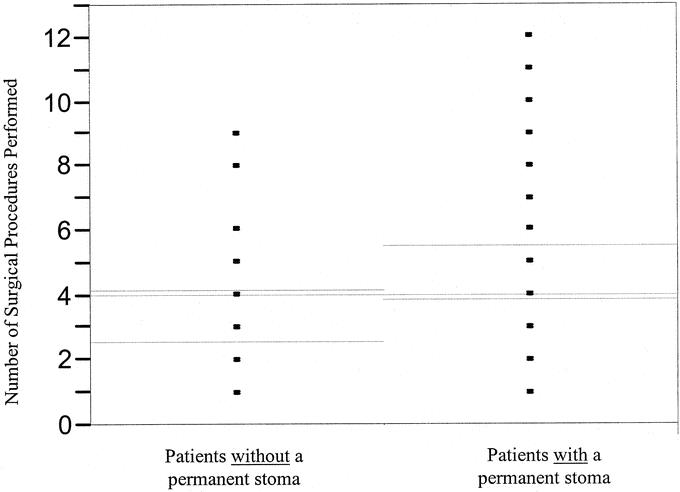
Results: CD associated with perianal CD was limited to the small bowel and/or ileocolic area in 23% of patients; the remainder had colorectal CD. Eighty-six patients underwent 344 operations. Forty-two patients (49%) ultimately required permanent diversion; among them were 21 of 32 patients (66%) with anal stricture and 12 of 20 women (60%) with rectovaginal fistula. Univariate analyses of clinical variables were performed with respect to need for permanent fecal diversion. Significant univariate predictors were the presence of colonic CD (P = 0.0045, odds ratio [OR] 5.4), avoidance of ileocolic resection (P = 0.0147, OR 0.4), and the presence of an anal stricture (P = 0.0165, OR 3.0). In multivariate logistic regression, the presence of colonic disease and anal canal stricture were predictors of permanent diversion. The OR associated with the risk of permanent diversion in the presence of colonic disease and in the absence of anal stricture was 10 (P = 0.0345). In the presence of both colonic disease and anal canal stenosis, the OR associated with permanent stoma was 33 (P = 0.0023).
Conclusions: The management of perianal CD continues to be challenging. Roughly half of patients required permanent fecal diversion, which was even more frequently true for patients with colonic CD and anal stenosis. Recognizing these tendencies will assist both patients and surgeons in planning optimal treatment.
Figures
References
-
- American Gastroenterological Association medical position statement: perianal Crohn's disease. Gastroenterology. 2003;125:1503–1507. - PubMed
-
- Schwartz DA, Pemberton JH, Sandborn WJ. Diagnosis and treatment of perianal fistulas in Crohn disease. Ann Intern Med. 2001;135:906–918. - PubMed
-
- Lapidus A, Bernell O, Hellers G, et al. Clinical course of colorectal Crohn's disease: a 35-year follow-up study of 507 patients. Gastroenterology. 1998;114:1151–1160. - PubMed
-
- van Dongen LM, Lubbers EJ. Perianal fistulas in patients with Crohn's disease. Arch Surg. 1986;121:1187–1190. - PubMed
-
- Sandborn WJ, Fazio VW, Feagan BG, et al. AGA technical review on perianal Crohn's disease. Gastroenterology. 2003;125:1508–1530. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
