

Proposed revision of the esophageal cancer staging system to accommodate pathologic response (pP) following preoperative chemoradiation (CRT)
- PMID: 15849517
- PMCID: PMC1357136
- DOI: 10.1097/01.sla.0000161983.82345.85
Proposed revision of the esophageal cancer staging system to accommodate pathologic response (pP) following preoperative chemoradiation (CRT)
Abstract
Objective: To determine the impact of pathologic response following preoperative chemoradiation (CRT) on the AJCC esophageal cancer staging system.
Summary background data: Increasing numbers of locoregionally advanced esophageal cancer patients are treated with preoperative CRT prior to surgical resection.
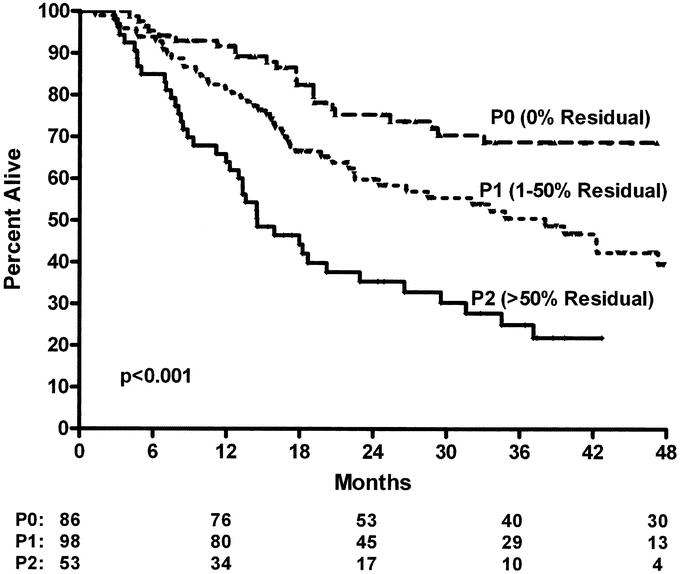
Methods: Five hundred ninety-three pts from 1985 to 2003 with esophageal cancer who underwent surgery with (n = 239) or without CRT (n = 354) were reviewed. Resected esophageal tumors were assessed for pathologic response by determining extent of residual tumor following CRT (P0, 0% residual; P1, 1%-50% residual; P2, >50% residual).
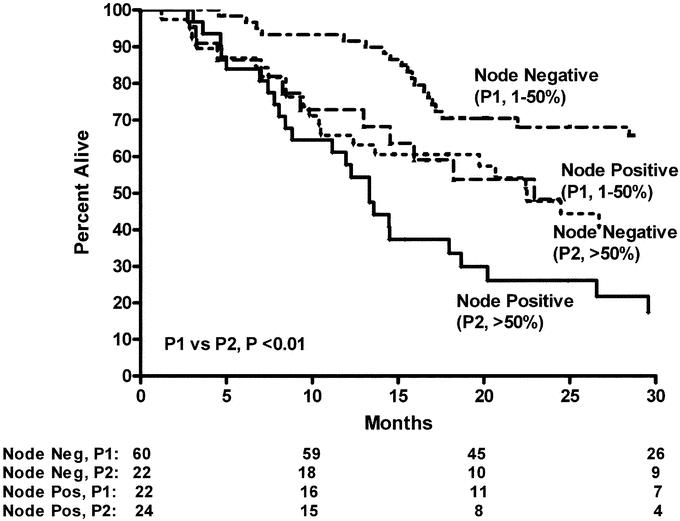
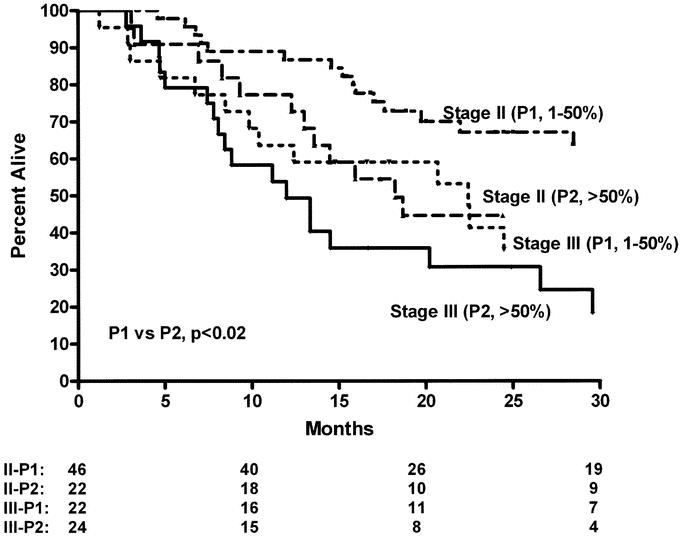
Results: After CRT down-staging, pTNM specific survival was similar, irrespective of treatment group (P = 0.98). The pTNM stage distribution was more favorable in the CRT group (P < 0.001) despite a more advanced initial cTNM stage distribution (P < 0.001). Following CRT, the pathologic response (pP) at the primary tumor as defined by extent of residual tumor predicted overall survival (3 years: P0, 0% residual = 74%; P1, 1%-50% residual = 54%; P2, >50% residual = 24%, P < 0.001) and stage specific survival with greater accuracy than pTNM stage alone.
Conclusions: Our analyses demonstrate that following CRT, pTNM continues to predict survival. The extent of pathologic response following CRT is an independent risk factor for survival (pP) and should be incorporated in the pTNM esophageal cancer staging system to better predict patient outcome in esophageal cancer.
Figures
References
-
- Muller JM, Erasmi H, Stelzner M, et al. Surgical therapy of oesophageal carcinoma. Br J Surg. 1990;77:845–857. - PubMed
-
- Hulscher JBF, van Sandick JW, de Boer AGEM, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med. 2002;347:1662–1669. - PubMed
-
- Walsh TN, Noonan N, Hollywood D, et al. A comparison of multimodal therapy and surgery for esophageal adenocarcinoma. N Engl J Med. 1996;335:462–467. - PubMed
-
- Urba SG, Orringer MB, Turrisi A, et al. Randomized trial of preoperative chemoradiation versus surgery alone in patients with locoregional esophageal carcinoma. J Clin Oncol. 2001;19:305–313. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
