

Impact of obesity on resource utilization for general surgical procedures
- PMID: 15849518
- PMCID: PMC1357137
- DOI: 10.1097/01.sla.0000161044.20857.24
Impact of obesity on resource utilization for general surgical procedures
Abstract
Objective: To determine the impact of the obesity epidemic on workload for general surgeons.
Summary background data: In 2001, the prevalence of obesity in the United States reached 26%, more than double the rate in 1990. This study focuses on the impact of obesity on surgical practice and resource utilization.
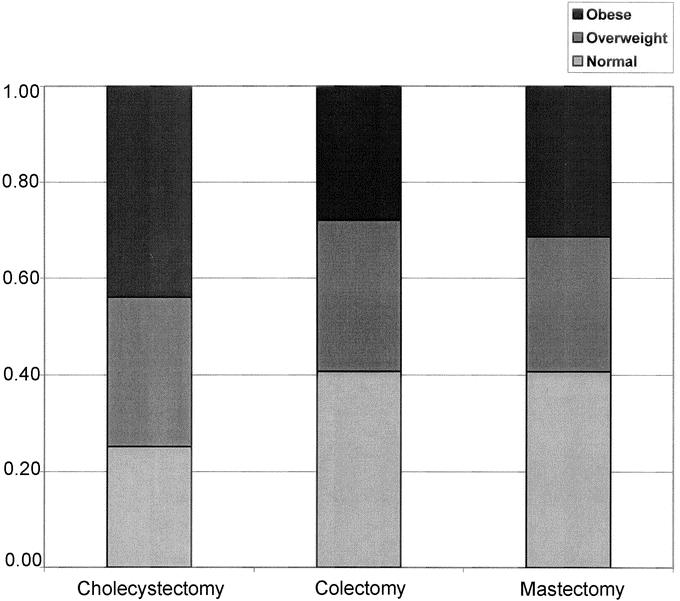
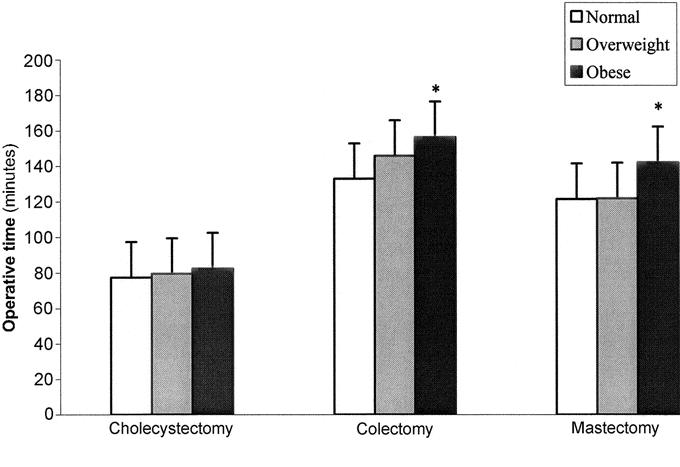
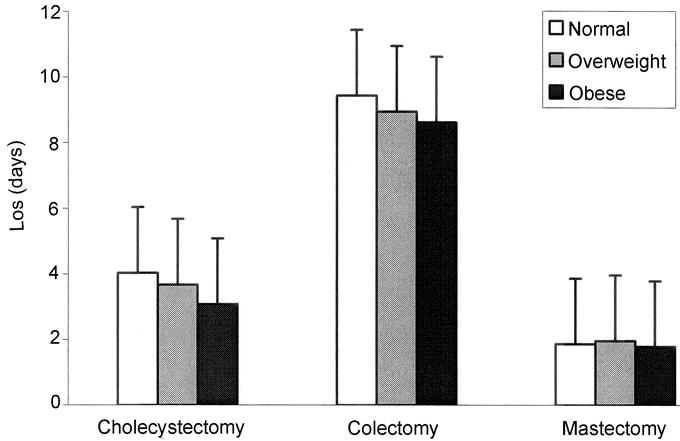
Methods: A retrospective analysis was done on patients undergoing cholecystectomy, unilateral mastectomy, and colectomy from January 2000 to December 2003 at a tertiary care center. The main outcome variables were operative time (OT), length of stay (LOS), and complications. The key independent variable was body mass index. We analyzed the association of obesity status with OT, LOS, and complications for each surgery, using multivariate regression models controlling for surgeon time-invariant characteristics.
Results: There were 623 cholecystectomies, 322 unilateral mastectomies, and 430 colectomies suitable for analysis from 2000 to 2003. Multivariable regression analyses indicated that obese patients had statistically significantly longer OT (P < 0.01) but not longer LOS (P > 0.05) or more complications (P > 0.05). Compared with a normal-weight patient, an obese patient had an additional 5.19 (95% confidence interval [CI], 0.15-10.24), 23.67 (95% CI, 14.38-32.96), and 21.42 (95% CI, 9.54-33.30) minutes of OT with respect to cholecystectomy, unilateral mastectomy, and colectomy. These estimates were robust in sensitivity analyses.
Conclusions: Obesity significantly increased OT for each procedure studied. These data have implications for health policy and surgical resource utilization. We suggest that a CPT modifier to appropriately reimburse surgeons caring for obese patients be considered.
Figures
References
-
- Mokdad AH, et al. Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA. 2003;289:76–79. - PubMed
-
- Mokdad AH, et al. Actual causes of death in the United States, 2000. JAMA. 2004;291:1238–1245. - PubMed
-
- Finkelstein EA, Fiebelkorn IC, Wang G. National medical spending attributable to overweight and obesity: how much, and who's paying? Health Aff (Millwood). 2003;suppl:W3-219–226. - PubMed
-
- Zizza CA, et al. Obesity affects nursing-care facility admission among whites but not blacks. Obes Res. 2002;10:816–823. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
