

Lower cancer incidence in Amsterdam-I criteria families without mismatch repair deficiency: familial colorectal cancer type X
- PMID: 15855431
- PMCID: PMC2933042
- DOI: 10.1001/jama.293.16.1979
Lower cancer incidence in Amsterdam-I criteria families without mismatch repair deficiency: familial colorectal cancer type X
Abstract
Context: Approximately 60% of families that meet the Amsterdam-I criteria (AC-I) for hereditary nonpolyposis colorectal cancer (HNPCC) have a hereditary abnormality in a DNA mismatch repair (MMR) gene. Cancer incidence in AC-I families with MMR gene mutations is reported to be very high, but cancer incidence for individuals in AC-I families with no evidence of an MMR defect is unknown.
Objective: To determine if cancer risks in AC-I families with no apparent deficiency in DNA MMR are different from cancer risks in AC-I families with DNA MMR abnormalities.
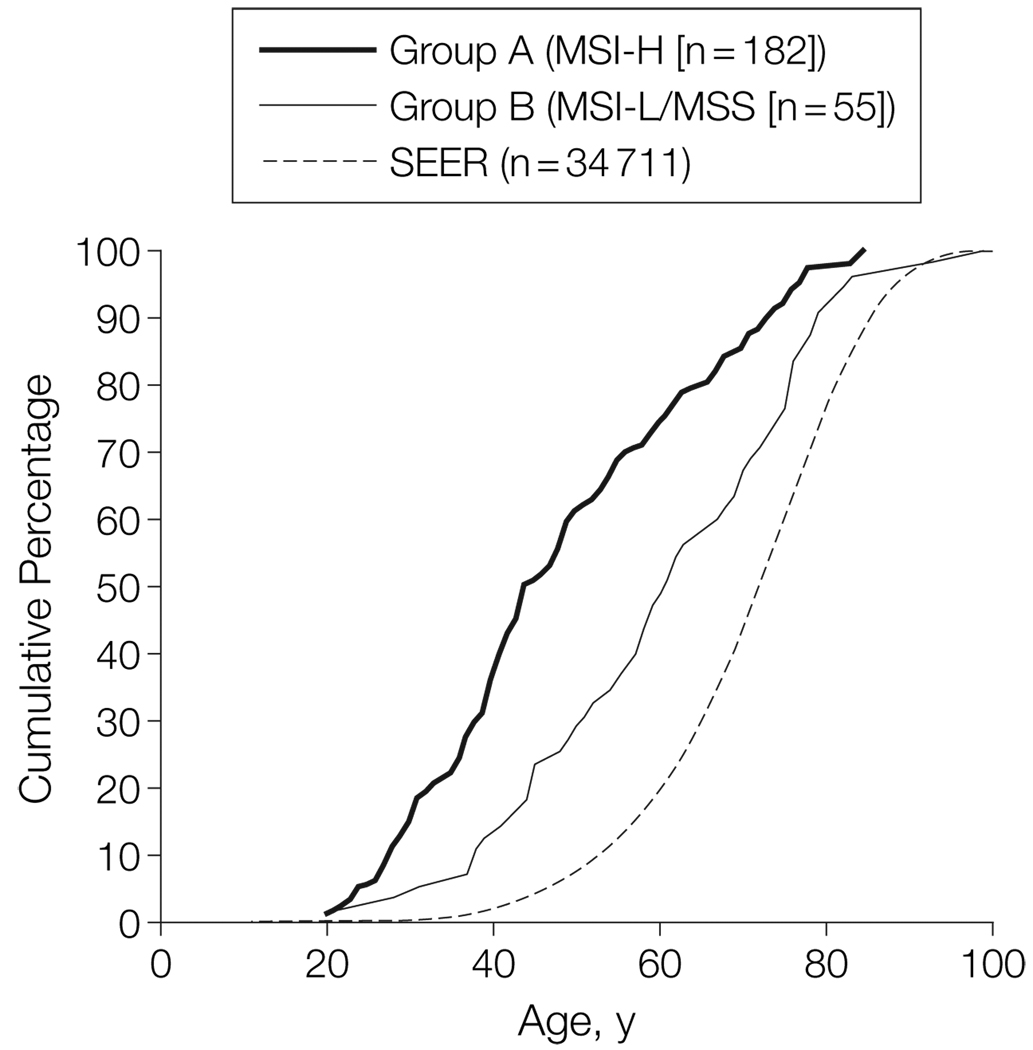
Design, setting, and participants: Identification (1997-2001) of 161 AC-I pedigrees from multiple population- and clinic-based sources in North America and Germany, with families grouped into those with (group A) or without (group B) MMR deficiency by tumor testing. A total of 3422 relatives were included in the analyses.
Main outcome measures: Cancer incidence in groups A and B (excluding the 3 affected members used to define each pedigree as AC-I) and computed age- and sex-adjusted standardized incidence ratios (SIRs) using Surveillance, Epidemiology, and End Results data.
Results: Group A families from both population- and clinic-based series showed increased incidence of the HNPCC-related cancers. Group B families showed increased incidence only for colorectal cancer (SIR, 2.3; 95% confidence interval, 1.7-3.0) and to a lesser extent than group A (SIR, 6.1; 95% confidence interval, 5.2-7.2) (P<.001).
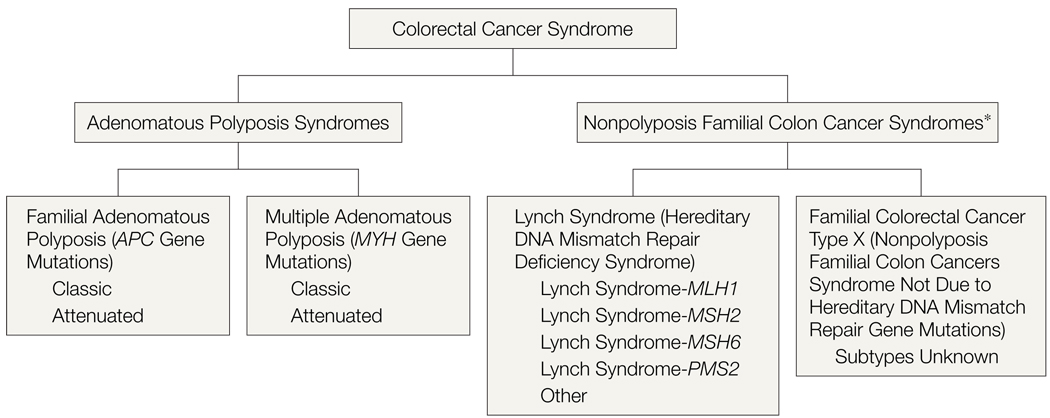
Conclusions: Families who fulfill AC-I criteria but who have no evidence of a DNA MMR defect do not share the same cancer incidence as families with HNPCC-Lynch syndrome (ie, hereditary MMR deficiency). Relatives in such families have a lower incidence of colorectal cancer than those in families with HNPCC-Lynch syndrome, and incidence may not be increased for other cancers. These families should not be described or counseled as having HNPCC-Lynch syndrome. To facilitate distinguishing these entities, the designation of "familial colorectal cancer type X" is suggested to describe this type of familial aggregation of colorectal cancer.
Figures
Comment in
-
Progress in genetic testing, classification, and identification of Lynch syndrome.JAMA. 2005 Apr 27;293(16):2028-30. doi: 10.1001/jama.293.16.2028. JAMA. 2005. PMID: 15855438 No abstract available.
-
Regarding the Clinical Practice Guidelines for the Surgical Treatment of Patients With Lynch Syndrome.Dis Colon Rectum. 2017 Jul;60(7):e595-e596. doi: 10.1097/DCR.0000000000000837. Dis Colon Rectum. 2017. PMID: 28594729 No abstract available.
-
The Authors Reply.Dis Colon Rectum. 2017 Jul;60(7):e596-e597. doi: 10.1097/DCR.0000000000000838. Dis Colon Rectum. 2017. PMID: 28594730 No abstract available.
References
-
- Watson P, Lynch H. Extracolonic cancer in hereditary nonpolyposis colorectal cancer. Cancer. 1993;71:677–685. - PubMed
-
- Aarnio M, Sankila R, Pukkala E, et al. Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int J Cancer. 1999;81:214–218. - PubMed
-
- Burke W, Petersen G, Lynch P, et al. Cancer Genetics Studies Consortium. Recommendations for follow-up care of individuals with an inherited predisposition to cancer, I: hereditary nonpolyposis colon cancer. JAMA. 1997;277:915–919. - PubMed
-
- Jarvinen HJ, Aarnio M. Surveillance on mutation carriers of DNA mismatch repair genes. Ann Chir Gynaecol. 2000;89:207–210. - PubMed
-
- Smith RA, Von Eschenbach AC, Wender R, et al. American Cancer Society. American Cancer Society guidelines for the early detection of cancer, 2004. CA Cancer J Clin. 2004;54:41–52. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 CA074799/CA/NCI NIH HHS/United States
- UO1 CA074800/CA/NCI NIH HHS/United States
- UO1 CA074799/CA/NCI NIH HHS/United States
- U01 CA074794/CA/NCI NIH HHS/United States
- UO1 CA074806/CA/NCI NIH HHS/United States
- UO1 CA078296/CA/NCI NIH HHS/United States
- U01 CA097735/CA/NCI NIH HHS/United States
- U01 CA074783/CA/NCI NIH HHS/United States
- UO1 CA074794/CA/NCI NIH HHS/United States
- CA-95-011/CA/NCI NIH HHS/United States
- U01 CA074806/CA/NCI NIH HHS/United States
- U24 CA074800/CA/NCI NIH HHS/United States
- U01 CA078296/CA/NCI NIH HHS/United States
- U01 CA074800/CA/NCI NIH HHS/United States
- UO1 CA097735/CA/NCI NIH HHS/United States
- UO1 CA074783/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
