

Microsatellite instability in colorectal cancer is associated with local lymphocyte infiltration and low frequency of distant metastases
- PMID: 15856045
- PMCID: PMC2362037
- DOI: 10.1038/sj.bjc.6602534
Microsatellite instability in colorectal cancer is associated with local lymphocyte infiltration and low frequency of distant metastases
Abstract
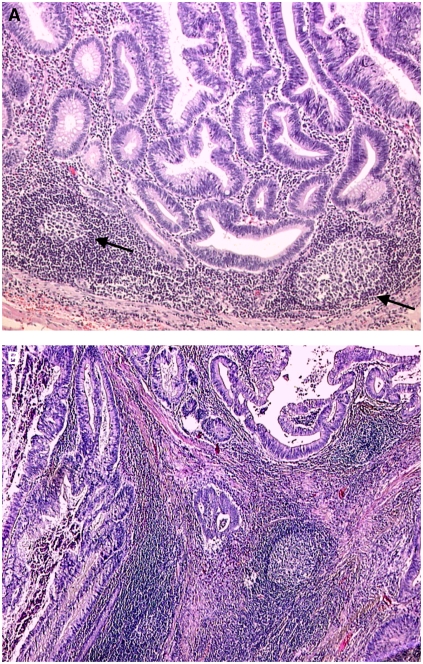
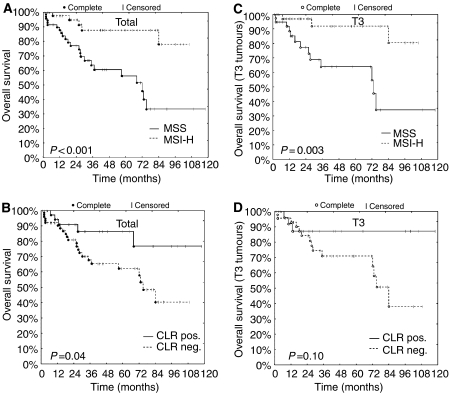
Colorectal carcinomas (CRCs) with high microsatellite instability (MSI-H) share clinicopathological features distinctly different from their microsatellite stable (MSS) counterparts. Unlike MSS cancers, MSI-H CRCs occur predominantly in the right-sided colon and are often characterised by a strong lymphocyte infiltration. A poor differentiation pattern is found in most MSI-H CRCs, even though patients with MSI-H carcinomas seem to have a significantly longer survival after surgical resection. To clarify which factors contribute to the obvious paradoxon of a more favourable prognosis of MSI tumours, several clinical and histopathological features as well as the microsatellite status were evaluated in 120 colorectal cancer cases fulfilling clinical criteria (Bethesda) indicative for familial colorectal cancer. Microsatellite instability status and lymphocyte infiltration were related to tumour stage and patients' follow-up. Statistical analysis confirmed well-known relations, such as enhanced lymphocyte infiltration accompanied by Crohn's like reaction (CLR) in MSI-H cancers (CLR+ in 27 out of 47 MSI-H vs 14 out of 71 MSS CRCs, P<0.001). However, after stratification for depth of local invasion and penetration of the primary tumour, T3 tumours displaying MSI had a significantly lower rate of distant metastases (M1 in four out of 35 MSI-H vs 20 out of 41 MSS CRCs, P<0.001). A similar tendency was observed for CLR-positive CRCs (M1 in six out of 29 CLR+ vs 17 out of 45 CLR- CRCs, P=0.13). In a logistic regression model, the MSI-H phenotype and the presence of CLR were independent predictors of a low UICC stage (P=0.006 and 0.04, respectively). These data, together with the recent definition of highly immunogenic neo-antigens expressed in MSI-H tumour cells, suggest that MSI-H CRCs elicit a protective host response that may prevent metastasis formation.
Figures
References
-
- Agresti A, Coull BA (1998) Approximate is better than ‘exact’ for interval estimation of binomial proportions. Am Stat 52: 119–126
-
- American Joint Committee on Cancer (1997) AJCC Cancer Staging Manual. Philadelphia: Lippincott-Raven
-
- Becker N (2003) [Epidemiology of colorectal cancer]. Radiologe 43: 98–104 - PubMed
-
- Boland CR (2000) Molecular genetics of hereditary nonpolyposis colorectal cancer. Ann N Y Acad Sci 910: 50–59, discussion 59–61 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
