

Do physicians know when their diagnoses are correct? Implications for decision support and error reduction
- PMID: 15857490
- PMCID: PMC1490097
- DOI: 10.1111/j.1525-1497.2005.30145.x
Do physicians know when their diagnoses are correct? Implications for decision support and error reduction
Abstract
Objective: This study explores the alignment between physicians' confidence in their diagnoses and the "correctness" of these diagnoses, as a function of clinical experience, and whether subjects were prone to over-or underconfidence.
Design: Prospective, counterbalanced experimental design.
Setting: Laboratory study conducted under controlled conditions at three academic medical centers.
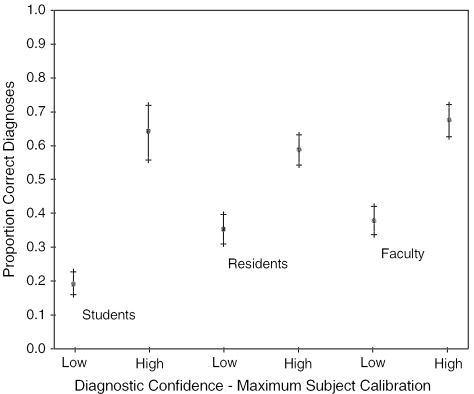
Participants: Seventy-two senior medical students, 72 senior medical residents, and 72 faculty internists.
Intervention: We created highly detailed, 2-to 4-page synopses of 36 diagnostically challenging medical cases, each with a definitive correct diagnosis. Subjects generated a differential diagnosis for each of 9 assigned cases, and indicated their level of confidence in each diagnosis.
Measurements and main results: A differential was considered "correct" if the clinically true diagnosis was listed in that subject's hypothesis list. To assess confidence, subjects rated the likelihood that they would, at the time they generated the differential, seek assistance in reaching a diagnosis. Subjects' confidence and correctness were "mildly" aligned (kappa=.314 for all subjects, .285 for faculty, .227 for residents, and .349 for students). Residents were overconfident in 41% of cases where their confidence and correctness were not aligned, whereas faculty were overconfident in 36% of such cases and students in 25%.
Conclusions: Even experienced clinicians may be unaware of the correctness of their diagnoses at the time they make them. Medical decision support systems, and other interventions designed to reduce medical errors, cannot rely exclusively on clinicians' perceptions of their needs for such support.
Figures
Comment in
-
The Causes of Errors in Clinical Reasoning: Cognitive Biases, Knowledge Deficits, and Dual Process Thinking.Acad Med. 2017 Jan;92(1):23-30. doi: 10.1097/ACM.0000000000001421. Acad Med. 2017. PMID: 27782919
References
-
- Hersh WR. A world of knowledge at your fingertips: the promise, reality, and future directions of online information retrieval. Acad Med. 1999;74:240–3. - PubMed
-
- Kohn LT, Corrigan JM, Donaldson MS, editors. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000. - PubMed
-
- Bates DW, Gawande AA. Error in medicine: what have we learned? Ann Intern Med. 2000;132:763–7. - PubMed
-
- Leape LL, Bates DW, Cullen DJ, et al. Systems analysis of adverse drug events. ADE Prevention Study Group. JAMA. 1995;274:35–43. - PubMed
-
- Wyatt JC. Clinical data systems, part 3: development and evaluation. Lancet. 1994;344:1682–7. - PubMed