

The impact of comorbidities on hormone use. After the 2000 release of the Women's Health Initiative
- PMID: 15857493
- PMCID: PMC1490092
- DOI: 10.1111/j.1525-1497.2005.04059.x
The impact of comorbidities on hormone use. After the 2000 release of the Women's Health Initiative
Abstract
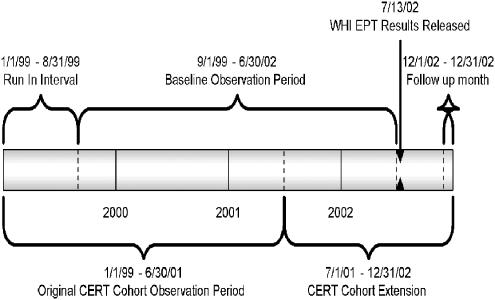
Objective: Determine the impact of fracture, coronary disease, and diabetes on changes in rates of discontinuation and initiation of estrogen therapy with (EPT) and without (ET) progestin, before (September 1, 1999 to June 30, 2002, baseline) versus 5 months after (follow-up) release of the Women's Health Initiative EPT trial results (WHI).
Design, setting, and participants: Observational cohort; 169,586 women 40 to 80 years old from 5 U.S. HMOs.
Methods: We used pharmacy data to identify ET and EPT users. A woman was a user any month she filled > or =1 estrogen prescription and in subsequent months based upon the number of pills/patches dispensed. We used inpatient and outpatient claims to identify fracture January 1, 1999 to June 30, 2002 and pharmacy data to identify disease-based groups of medications for diabetes and cardiovascular disease.
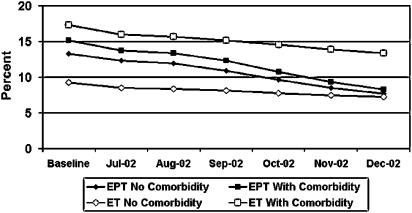
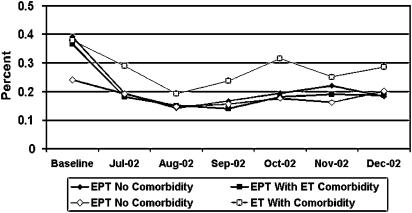
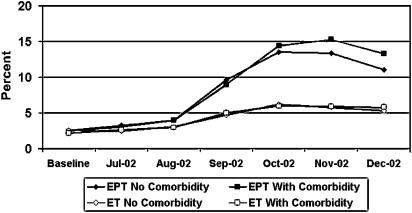
Measures: EPT/ET prevalence, initiation, and discontinuation rates.
Results: Baseline to follow-up EPT and ET prevalence declined 45% and 22%, respectively, with no difference by comorbidity. Follow-up EPT initiation was half the baseline rate irrespective of comorbidity. Compared to baseline, follow-up EPT discontinuation rates increased among women with diabetes (relative risk [RR], 6.9; 95% confidence interval [CI], 5.6 to 8.4), cardiovascular disease (RR, 5.5; 95% CI, 4.9 to 6.2), fracture (RR, 3.8; 95% CI, 2.4 to 5.7), and no comorbidity (RR, 4.4; 95% CI, 3.9 to 4.9). The RRs for follow-up versus baseline EPT discontinuation were higher among women with diabetes (P<.01) and cardiovascular disease (P<.01) versus women without these comorbidities. ET discontinuation rates among these same groups were elevated 2- to 2.8-fold.
Conclusions: Diabetes and cardiovascular disease were associated with higher EPT discontinuation rates post-WHI compared to women without comorbidity; comorbidity had little impact on changes in prevalence or initiation of ET/EPT after release of the WHI.
Figures
References
-
- Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women's Health Initiative randomized controlled trial. JAMA. 2002;288:321–33. - PubMed
-
- Shumaker SA, Legault C, Rapp SR, et al. Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in postmenopausal women: the Women's Health Initiative Memory Study: a randomized controlled trial. JAMA. 2003;289:2651–62. - PubMed
-
- Rapp SR, Espeland MA, Shumaker SA, et al. Effect of estrogen plus progestin on global cognitive function in postmenopausal women: the Women's Health Initiative Memory Study: a randomized controlled trial. JAMA. 2003;289:2663–72. - PubMed
-
- Chlebowski RT, Hendrix SL, Langer RD, et al. Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the Women's Health Initiative Randomized Trial. JAMA. 2003;289:3243–53. - PubMed
-
- Hays J, Ockene JK, Brunner RL, et al. Effects of estrogen plus progestin on health-related quality of life. N Engl J Med. 2003;348:1839–54. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical