

Lack of association between Chlamydia Pneumoniae serology and endothelial dysfunction of coronary arteries
- PMID: 15857519
- PMCID: PMC1097745
- DOI: 10.1186/1476-7120-3-12
Lack of association between Chlamydia Pneumoniae serology and endothelial dysfunction of coronary arteries
Abstract
Background: Recent publications brought up the hypothesis that an infection with Chlamydia Pneumoniae (CP) might be a major cause of coronary artery disease (CAD). Therefore, we investigated whether endothelial dysfunction (ED) as a precursor of atherosclerosis might be detectable in patients with previous infection with CP but without angiographic evidence of CAD.
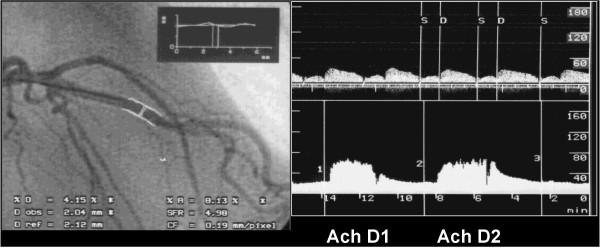
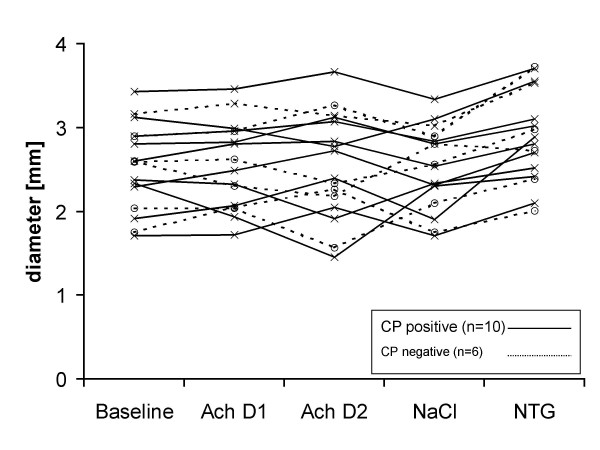
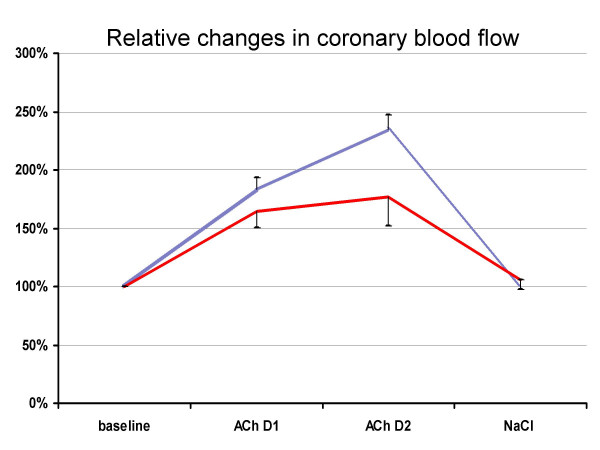
Methods: We included 16 patients (6 male / 10 female) of 52 consecutive patients with normal coronary angiography who had typical angina pectoris and pathologic findings in the stress test. Exclusion criteria were: active smoker, elevated cholesterol, hypertension, age > 65 years, diabetes mellitus, treatment with ACE-inhibitors, or known CAD. Blood sample analysis for serum titer against CP (aCP-IgG) was performed after coronary angiography. We looked for endothelial dysfunction analyzing the diameter of the left anterior descending coronary artery (LAD) before and after acetylcholine (ACh) i. c. Quantitative analysis of luminal diameter (LD) was performed in at least two planes during baseline conditions and after ACh for 2 minutes in dosages of 7.2 microg/min and 36 microg/min with an infusion speed of 2 ml/min. Using Doppler guide wire, the coronary flow velocity was measured continuously in the LAD. The coronary flow velocity reserve (CFVR) was measured after 20 microg adenosine i. c.
Results: 10 patients had an elevated aCP-IgG (> 1:8). 6 patients with negative titers (aCP-IgG <or= 1:8) served as control (CTRL). Both groups were comparable in age, gender, angina class, results of non-invasive stress-test and the baseline values of LD and flow. In the CP positive group 3 patients (30%) did not show an increase of LD after ACh as evidence of ED. In the CTRL group 4 patients (67 %) had ED. There was no association between aCP-IgG and changes of coronary blood flow after ACh. All patients showed normal CFVR (3.0 +/- 0.27) irrespective of their aCP-IgG values.
Conclusion: In patients with typical symptoms of coronary ischemia but without angiographically visible CAD and absence of other factors affecting the endothelial function, a previous infection with CP is not associated with endothelial dysfunction.
Figures
Similar articles
-
The relationship between Chlamydophila pneumoniae IgG titer and coronary atherosclerosis.Cardiol J. 2008;15(3):245-51. Cardiol J. 2008. PMID: 18651417
-
Relationship between endothelial function in the coronary and brachial arteries.Clin Cardiol. 2005 Oct;28(10):460-6. doi: 10.1002/clc.4960281004. Clin Cardiol. 2005. PMID: 16274093 Free PMC article.
-
Transthoracic coronary flow velocity reserve assessment: comparison between adenosine and dobutamine.J Am Soc Echocardiogr. 2006 Oct;19(10):1220-8. doi: 10.1016/j.echo.2006.04.028. J Am Soc Echocardiogr. 2006. PMID: 17000360 Clinical Trial.
-
Pathogenesis of atherosclerosis: a possible relation to infection.Atherosclerosis. 1998 Oct;140 Suppl 1:S3-9. doi: 10.1016/s0021-9150(98)00113-0. Atherosclerosis. 1998. PMID: 9859918 Review.
-
Microbubble-endothelial cell interactions as a basis for assessing endothelial function.Echocardiography. 2002 Jul;19(5):427-38. doi: 10.1046/j.1540-8175.2002.00427.x. Echocardiography. 2002. PMID: 12174207 Review.
Cited by
-
Persistence of an atherogenic lipid profile after treatment of acute infection with Brucella.J Lipid Res. 2009 Dec;50(12):2532-9. doi: 10.1194/jlr.P900063-JLR200. Epub 2009 Jun 17. J Lipid Res. 2009. PMID: 19535817 Free PMC article. Clinical Trial.
-
Circulating endothelial progenitor cells are not affected by acute systemic inflammation.Am J Physiol Heart Circ Physiol. 2010 Jun;298(6):H2054-61. doi: 10.1152/ajpheart.00921.2009. Epub 2010 Apr 9. Am J Physiol Heart Circ Physiol. 2010. PMID: 20382859 Free PMC article. Clinical Trial.
-
Association of Chlamydia trachomatis, C. pneumoniae, and IL-6 and IL-8 Gene Alterations With Heart Diseases.Front Immunol. 2019 Feb 5;10:87. doi: 10.3389/fimmu.2019.00087. eCollection 2019. Front Immunol. 2019. PMID: 30804931 Free PMC article.
References
-
- Persson K. Epidemiological and clinical aspects on infections due to Chlamydia pneumoniae (strain TWAR) Scand J Infect Dis Suppl. 1990;69:63–67. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
