

Management of leiomyosarcomas of the spermatic cord: the role of reconstructive surgery
- PMID: 15860129
- PMCID: PMC1097762
- DOI: 10.1186/1477-7819-3-23
Management of leiomyosarcomas of the spermatic cord: the role of reconstructive surgery
Abstract
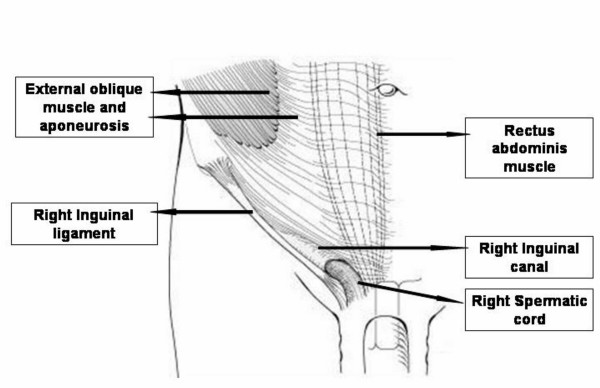
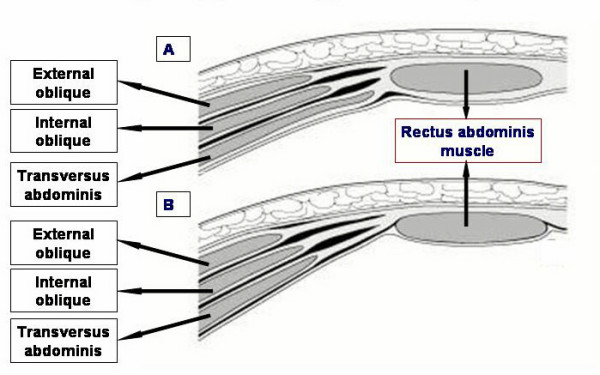
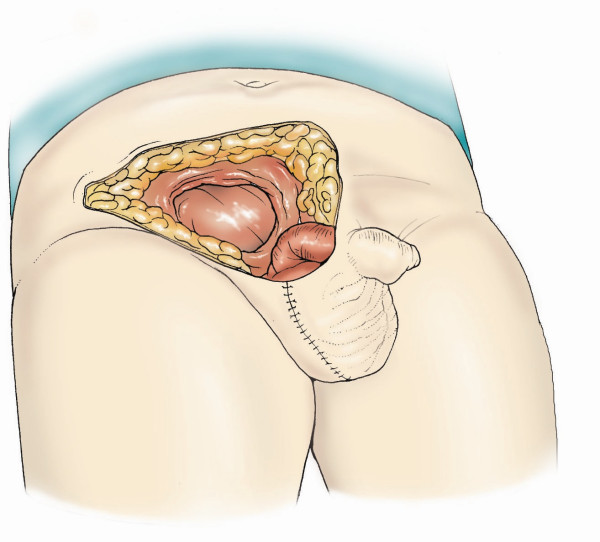
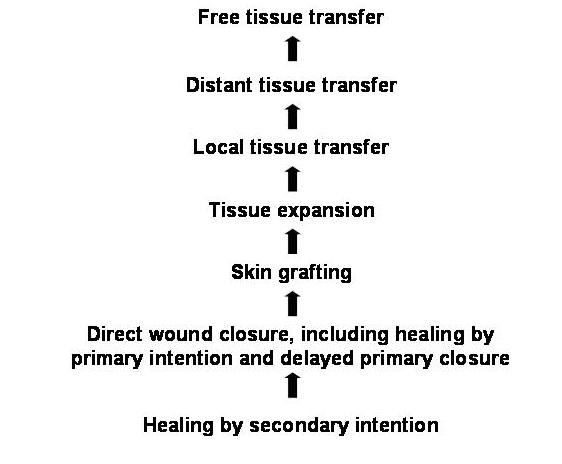
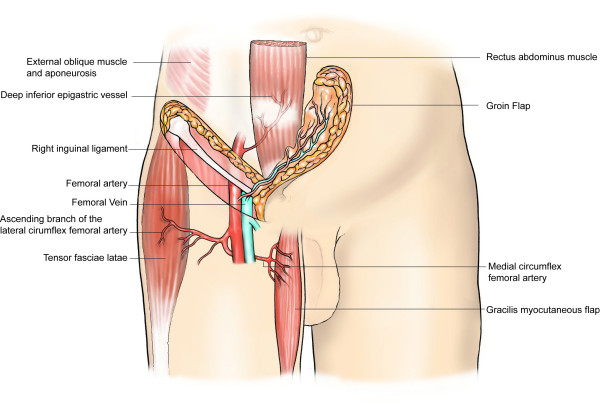
BACKGROUND: Leiomyosarcomas (LMS) of the spermatic cord are extremely rare. Radical inguinal orchiectomy and high ligation of the cord is the standard primary surgical procedure. The extent of surrounding soft tissue excision required and the precise role of adjuvant radiotherapy, however, remains unclear. In addition, recurrence is a commonly encountered problem which might necessitate further radical excision of adjacent soft tissues. METHODS: This article reviews the pathophysiology of spermatic cord leiomyosarcomas (LMS), and discusses the various reconstructive surgical options available to repair the inguinal region and the lower anterior abdominal wall after excision of the tumour and the adjacent soft tissues. RESULTS: There is paucity of literature on LMS of spermatic cord. The majority of paratesticular neoplasms are of mesenchymal origin and up to 30% of these are malignant. In adults, approximately 10% of spermatic cord sarcomas are LMS. Approximately 50% of these tumours recur loco-regionally following definitive surgery; however, the incidence decreases if resection is followed by adjuvant radiotherapy. CONCLUSION: It is therefore important to achieve negative histological margins during the primary surgical procedure, even if adjuvant radiotherapy is instituted. If extensive resection is required, either during the primary procedure or following recurrence, reconstructive surgery may become necessary. This article reviews the pathophysiology of spermatic cord LMS, the reasons for recurrence, and discusses the management options including the role of reconstructive surgery.
Figures
References
-
- Lioe TF, Biggart JD. Tumours of the spermatic cord and paratesticular tissue. A clinicopathologic study. Br J Urol. 1993;71:600–606. - PubMed
-
- Donovan MG, Fitzpatrick JM, Gaffney EF. Paratesticular leiomyosarcoma. Br J Urol. 1987;60:590. - PubMed
-
- Bajaj P, Agarwal K, Niveditha SR, Pathania OP. Leiomyosarcoma arising from tunica vaginalis testis: a case report. Indian J Pathol Microbiol. 2001;44:145–146. - PubMed
-
- Rao CR, Srinivasulu M, Naresh KN, Doval DC, Hazarika D. Adult Paratesticular Sarcomas: A report of eight cases. J Surg Oncol. 1994;56:89–93. - PubMed
-
- Padilla AJ, Gonzalez CM, Caldero MM, Arano YA, Torroella BF, Fanlo AP. Leiomyosarcoma of the spermatic cord. Actas Urol Esp. 1993;17:464–467. - PubMed
LinkOut - more resources
Full Text Sources
