

Early efficacy of CABG care delivery in a low procedure-volume community hospital: operative and midterm results
- PMID: 15865623
- PMCID: PMC1131908
- DOI: 10.1186/1471-2482-5-10
Early efficacy of CABG care delivery in a low procedure-volume community hospital: operative and midterm results
Abstract
Background: The Leapfrog Group recommended that coronary artery bypass grafting (CABG) surgery should be done at high volume hospitals (>450 per year) without corresponding surgeon-volume criteria. The latter confounds procedure-volume effects substantially, and it is suggested that high surgeon-volume (>125 per year) rather than hospital-volume may be a more appropriate indicator of CABG quality.
Methods: We assessed 3-year isolated CABG morbidity and mortality outcomes at a low-volume hospital (LVH: 504 cases) and compared them to the corresponding Society of Thoracic Surgeons (STS) national data over the same period (2001-2003). All CABGs were performed by 5 high-volume surgeons (161-285 per year). "Best practice" care at LVH -- including effective practice guidelines, protocols, data acquisition capabilities, case review process, dedicated facilities and support personnel -- were closely modeled after a high-volume hospital served by the same surgeon-team.
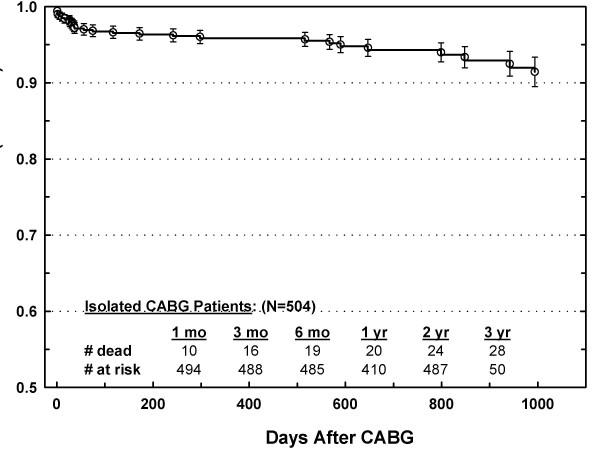
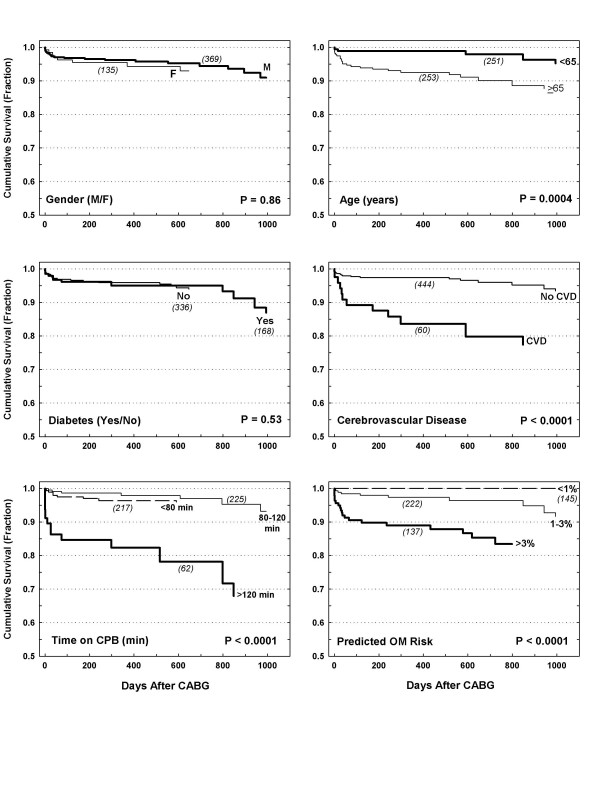
Results: Operative mortality was similar for LVH and STS (OM: 2.38% vs. 2.53%), and the corresponding LVH observed-to-expected mortality (O/E = 0.81) indicated good quality relative to the STS risk model (O/E<1). Also, these results were consistent irrespective of risk category: O/E was 0, 0.9 and 1.03 for very-low risk (<1%), low risk (1-3%) and moderate-to-high risk category (>3%), respectively. Postoperative leg wound infections, ventilator hours, renal dysfunction (no dialysis), and atrial fibrillation were higher for LVH, but hospital stay was not. The unadjusted Kaplan-Meier survival for the LVH cohort was 96%, 94%, and 92% at one, two, and three years, respectively.
Conclusion: Our results demonstrated that high quality CABG care can be achieved at LVH programs if 1) served by high volume surgeons and 2) patient care procedures similar to those of large programs are implemented. This approach may prove a useful paradigm to ensure high quality CABG care and early efficacy at low volume institutions that wish to comply with the Leapfrog standards.
Figures
Similar articles
-
Is hospital procedure volume a reliable marker of quality for coronary artery bypass surgery? A comparison of risk and propensity adjusted operative and midterm outcomes.Ann Thorac Surg. 2005 Jun;79(6):1961-9. doi: 10.1016/j.athoracsur.2004.12.002. Ann Thorac Surg. 2005. PMID: 15919292
-
The "occasional open heart surgeon" revisited.J Thorac Cardiovasc Surg. 2008 Jun;135(6):1254-60. doi: 10.1016/j.jtcvs.2007.10.077. J Thorac Cardiovasc Surg. 2008. PMID: 18544365
-
Impact of patient risk on the hospital volume-outcome relationship in coronary artery bypass grafting.Arch Intern Med. 2005 Feb 14;165(3):333-7. doi: 10.1001/archinte.165.3.333. Arch Intern Med. 2005. PMID: 15710799
-
How valid is the quantity and quality relationship in CABG surgery? A review of the literature.J Card Surg. 2010 Nov;25(6):713-8. doi: 10.1111/j.1540-8191.2010.01146.x. Epub 2010 Oct 11. J Card Surg. 2010. PMID: 21044159 Review.
-
Quality-of-care indicators for oesophageal cancer surgery: A review.Eur J Surg Oncol. 2010 Nov;36(11):1035-43. doi: 10.1016/j.ejso.2010.08.131. Epub 2010 Sep 16. Eur J Surg Oncol. 2010. PMID: 20846818 Review.
Cited by
-
Implementation of an antibiotic nomogram improves postoperative antibiotic utilization and safety in patients undergoing coronary artery bypass grafting.Patient Saf Surg. 2007 Nov 7;1(1):2. doi: 10.1186/1754-9493-1-2. Patient Saf Surg. 2007. PMID: 18271990 Free PMC article.
-
Risk factors for postoperative respiratory mortality and morbidity in patients undergoing coronary artery bypass grafting.Anesth Pain Med. 2012 Fall;2(2):60-5. doi: 10.5812/aapm.5228. Epub 2012 Sep 13. Anesth Pain Med. 2012. PMID: 24223339 Free PMC article. Review.
References
-
- Zelen J, Bilfinger TV, Anagnostopoulos CE. Coronary artery bypass grafting. The relationship of surgical volume, hospital location, and outcome. N Y State J Med. 1991;91:290–292. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
