

Perceived barriers for treatment of chronic heart failure in general practice; are they affecting performance?
- PMID: 15869704
- PMCID: PMC1131898
- DOI: 10.1186/1471-2296-6-19
Perceived barriers for treatment of chronic heart failure in general practice; are they affecting performance?
Abstract
Background: The aim of this study is to determine to what extent barriers perceived by general practitioners (GPs) for prescribing angiotensin-converting enzyme inhibitors (ACE-I) in chronic heart failure (CHF) patients are related to underuse and underdosing of these drugs in actual practice.
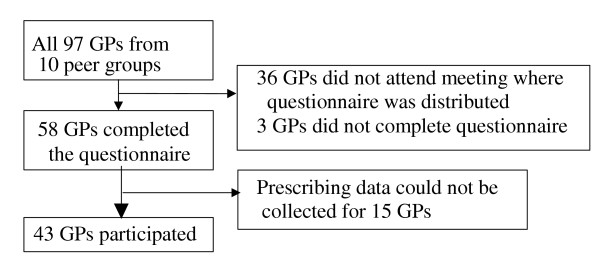
Methods: Barriers were assessed with a semi-structured questionnaire. Prescribing data were extracted from GPs' computerised medical records for a random sample of their CHF patients. Relations between barriers and prescribing behaviour were assessed by means of Spearman rank correlation and multivariate regression modelling.
Results: GPs prescribed ACE-I to 45% of their patients and had previously initiated such treatment in an additional 3.5%, in an average standardised dose of 13.5 mg. They perceived a median of four barriers in prescribing ACE-I or optimising ACE-I dose. Many GPs found it difficult to change treatment initiated by a cardiologist. Furthermore, initiating ACE-I in patients already using a diuretic or stable on their current medication was perceived as barrier. Titrating the ACE-I dose was seen as difficult by more than half of the GPs. No significant relationships could be found between the barriers perceived and actual ACE-I prescribing. Regarding ACE-I dosing, the few GPs who did not agree that the ACE-I should be as high as possible prescribed higher ACE-I doses.
Conclusion: Variation between GPs in prescribing ACE-I for CHF cannot be explained by differences in the barriers they perceive. Tailor-made interventions targeting only those doctors that perceive a specific barrier will therefore not be an efficient approach to improve quality of care.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
