

Incidence of stillbirth and perinatal mortality and their associated factors among women delivering at Harare Maternity Hospital, Zimbabwe: a cross-sectional retrospective analysis
- PMID: 15876345
- PMCID: PMC1156907
- DOI: 10.1186/1471-2393-5-9
Incidence of stillbirth and perinatal mortality and their associated factors among women delivering at Harare Maternity Hospital, Zimbabwe: a cross-sectional retrospective analysis
Abstract
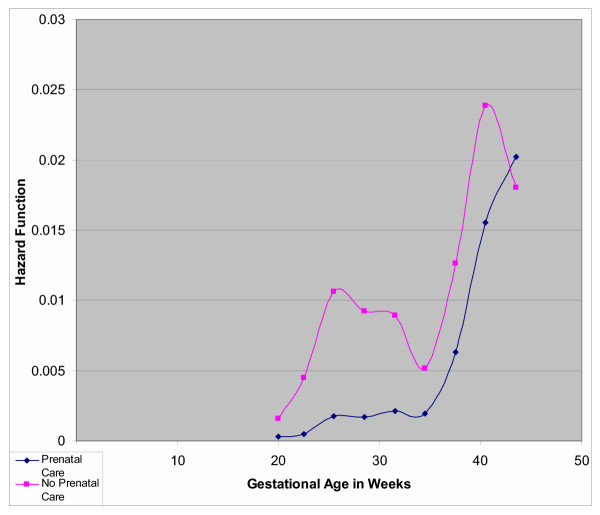
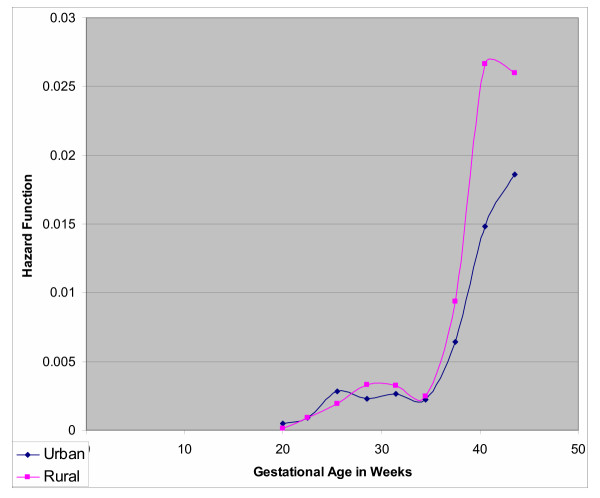
BACKGROUND: Death of an infant in utero or at birth has always been a devastating experience for the mother and of concern in clinical practice. Infant mortality remains a challenge in the care of pregnant women worldwide, but particularly for developing countries and the need to understand contributory factors is crucial for addressing appropriate perinatal health. METHODS: Using information available in obstetric records for all deliveries (17,072 births) at Harare Maternity Hospital, Zimbabwe, we conducted a cross-sectional retrospective analysis of a one-year data, (1997-1998) to assess demographic and obstetric risk factors for stillbirth and early neonatal death. We estimated risk of stillbirth and early neonatal death for each potential risk factor. RESULTS: The annual frequency of stillbirth was 56 per 1,000 total births. Women delivering stillbirths and early neonatal deaths were less likely to receive prenatal care (adjusted relative risk [RR] = 2.54; 95% confidence intervals [CI] 2.19-2.94 and RR = 2.52; 95% CI 1.63-3.91), which for combined stillbirths and early neonatal deaths increased with increasing gestational age (Hazard Ratio [HR] = 3.98, HR = 7.49 at 28 and 40 weeks of gestation, respectively). Rural residence was associated with risk of infant dying in utero, (RR = 1.33; 95% CI 1.12-1.59), and the risk of death increased with increasing gestational age (HR = 1.04, HR = 1.69, at 28 and 40 weeks of gestation, respectively). Older maternal age was associated with risk of death (HR = 1.50; 95% CI 1.21-1.84). Stillbirths were less likely to be delivered by Cesarean section (RR = 0.64; 95% CI 0.51-0.79), but more likely to be delivered as breech (RR = 4.65; 95% CI 3.88-5.57, as were early neonatal deaths (RR = 3.38; 95% CI 1.64-6.96). CONCLUSION: The frequency of stillbirth, especially macerated, is high, 27 per 1000 total births. Early prenatal care could help reduce perinatal death linking the woman to the health care system, increasing the probability that she would seek timely emergency care that would reduce the likelihood of death of her infant in utero. Improved quality of obstetric care during labor and delivery may help reduce the number of fresh stillbirths and early neonatal deaths.
Figures
References
-
- Kramer MS. The Epidemiology of Adverse Pregnancy Outcomes; An Overview. J Nutr. 2003;133:1592S–1596S. - PubMed
-
- Kumar MR, Bhat BV, Oumachigui A. Perinatal mortality trends in a referral hospital. Indian J Pediatr. 1996;63:357–361. - PubMed
-
- Kambarami RA. Levels and risk factors for mortality in infants with birth weights between 500 and 1800 grams in a developing country: a hospital based study. Cent Afr J Med. 2002;48:133–136. - PubMed
-
- Cnattingius S, Stephansson O. The Epidemiology of Stillbirth. Semin Perinatol. 2002;26:25–30. - PubMed
-
- Gardosi J, Mul T, Mongelli M, Fagan D. Analysis of birthweight and gestational age in antepartum stillbirths. Br J Obstet Gynaecol. 1998;105:524–530. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
