

Testosterone as a predictor of pathological stage in clinically localized prostate cancer
- PMID: 15879785
- PMCID: PMC1855287
- DOI: 10.1097/01.ju.0000158040.33531.e7
Testosterone as a predictor of pathological stage in clinically localized prostate cancer
Abstract
Purpose: Substantial controversy exists in the literature regarding the association between pretreatment testosterone and disease outcome in patients with prostate cancer. We explored the relationship between preoperative total testosterone, and pathological stage and progression in patients with clinically localized prostate cancer treated with radical prostatectomy.
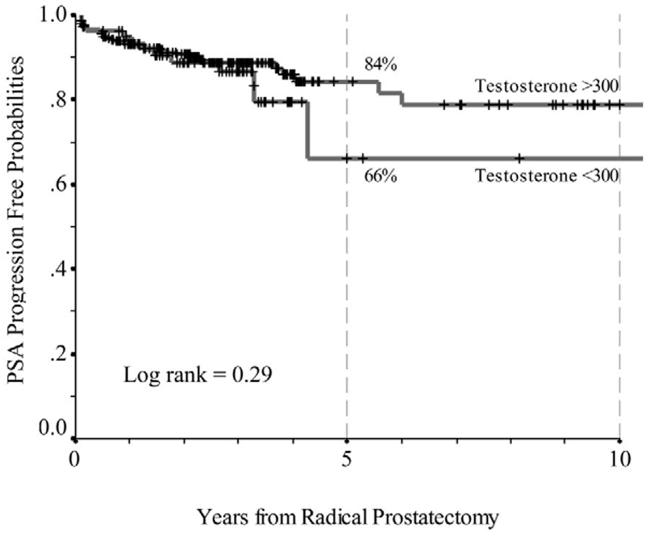
Materials and methods: We retrospectively reviewed the records of consecutive patients with clinically localized prostate cancer treated with radical prostatectomy between January 1990 and June 2003. A total of 326 patients with pretreatment testosterone levels available were eligible for this analysis. Biochemical progression (BCR) was defined by postoperative prostate specific antigen (PSA) greater than 0.4 ng/ml with a confirmatory increase and it occurred in 41 men. No men received adjuvant therapy. Univariate and multivariate logistic regression analyses were done to examine whether pretreatment testosterone was associated with pathological stage. Cox regression was used to assess the association of testosterone and BCR.
Results: Median PSA was 6.01 ng/ml (range 0.13 to 86), testosterone was 385 ng/dl (range 133 to 998) and followup was 36 months (range 4 to 136). In 245 patients (75%) disease was organ confined. Lower testosterone correlated with adverse pathological stage on multivariate analysis (p = 0.01), as did clinical stage, biopsy grade and PSA. However, we found no relationship between testosterone and BCR after adjusting for covariates. Furthermore, we found no evidence of an interaction between PSA and testosterone (p = 0.4).
Conclusions: On multivariate analysis low preoperative total testosterone was associated with advanced pathological stage but not with BCR. Future studies are warranted with data on more patients who have progressed.
Figures
References
-
- Prehn RT. On the prevention and therapy of prostate cancer by androgen administration. Cancer Res. 1999;59::4161. - PubMed
-
- Lucia MS, Bostwick DG, Bosland M, Cockett AT, Knapp DW, Leav I, et al. Workgroup I: rodent modelsof prostate cancer. Prostate. 1998;36::49. - PubMed
-
- Bladou F, Vessella RL, Buhler KR, Ellis WJ, True LD, Lange PH. Cell proliferation and apoptosis during prostatic tumor xenograft involution and regrowth after castration. Int J Cancer. 1996;67::785. - PubMed
-
- Stattin P, Lumme S, Tenkanen L, Alfthan H, Jellum E, Hallmans G, et al. High levels of circulating testosterone are not associated with increased prostate cancer risk: a pooled prospective study. Int J Cancer. 2004;108::418. - PubMed
-
- Gann PH, Hennekens CH, Ma J, Longcope C, Stampfer MJ. Prospective study of sex hormone levels and risk of prostate cancer. J Natl Cancer Inst. 1996;88::1118. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
