

Thrombolysis for acute ischemic stroke: results of the Canadian Alteplase for Stroke Effectiveness Study
- PMID: 15883405
- PMCID: PMC557101
- DOI: 10.1503/cmaj.1041561
Thrombolysis for acute ischemic stroke: results of the Canadian Alteplase for Stroke Effectiveness Study
Abstract
Background: Thrombolysis for acute ischemic stroke has remained controversial. The Canadian Alteplase for Stroke Effectiveness Study, a national prospective cohort study, was conducted to assess the effectiveness of alteplase therapy for ischemic stroke in actual practice.
Methods: The study was mandated by the federal government as a condition of licensure of alteplase for the treatment of stroke in Canada. A registry was established to collect data over 2.5 years for stroke patients receiving such treatment from Feb. 17, 1999, through June 30, 2001. All centres capable of administering thrombolysis therapy according to Canadian guidelines were eligible to submit patient data to the registry. Data collection was prospective, and follow-up was completed at 90 days after stroke. Copies of head CT scans obtained at baseline and at 24-48 hours after the start of treatment were submitted to a central panel for review.
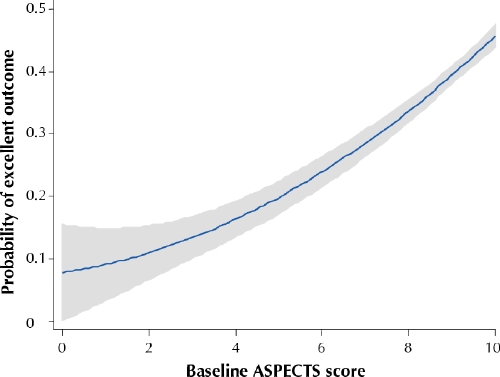
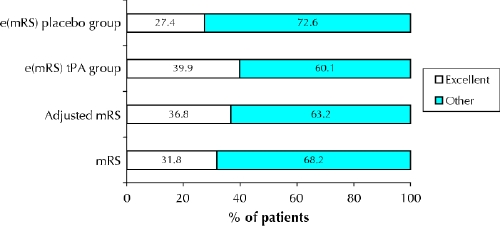
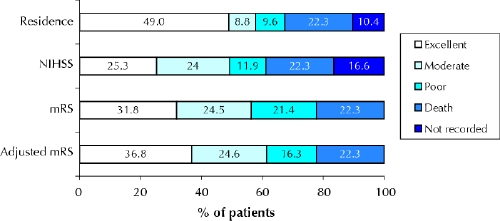
Results: A total of 1135 patients were enrolled at 60 centres in all major hospitals across Canada. The registry collected data for an estimated 84% of all treated ischemic stroke patients in the country. An excellent clinical outcome was observed in 37% of the patients. Symptomatic intracranial hemorrhage occurred in only 4.6% of the patients (95% confidence interval [CI] 3.4%-6.0%); however, 75% of these patients died in hospital. An additional 1.3% (95% CI 0.7%-2.2%) of patients had hemiorolingual angioedema.
Conclusions: The outcomes of stroke patients undergoing thrombolysis in Canada are commensurate with the results of clinical trials. The rate of symptomatic intracranial hemorrhage was low. Stroke thrombolysis is a safe and effective therapy in actual practice.
Figures
References
-
- Sussman BJ, Fitch TSP, Plainfield NJ. Thrombolysis with fibrinolysin in cerebral arterial occlusion. JAMA 1958;167:1705-9. - PubMed
-
- Meyer JS, Gilroy J, Barnhart MI, Johnson JF. Therapeutic thrombolysis in cerebral thromboembolism. Double-blind evaluation of intravenous plasmin therapy in carotid and middle cerebral artery occlusion. Neurology 1963;13: 927-37. - PubMed
-
- Del Zoppo GJ, Poeck K, Pessin MS, Wolpert SM, Furlan AJ, Ferbert A, et al. Recombinant tissue plasminogen activator in acute thrombotic and embolic stroke. Ann Neurol 1992;32:78-86. - PubMed
-
- Brott TG, Haley EC Jr, Levy DE, Barsan W, Broderick J, Sheppard GL, et al. Urgent therapy for stroke. Part I. Pilot study of tissue plasminogen activator administered within 90 minutes. Stroke 1992;23:632-40. - PubMed
-
- Haley EC Jr, Levy DE, Brott TG, Sheppard GL, Wong MC, Kongable GL, et al. Urgent therapy for stroke. Part II. Pilot study of tissue plasminogen activator administered 91–180 minutes from onset. Stroke 1992;23:641-5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical