

Patient defined dichotomous end points for remission and clinical improvement in ulcerative colitis
- PMID: 15888785
- PMCID: PMC1774553
- DOI: 10.1136/gut.2004.056358
Patient defined dichotomous end points for remission and clinical improvement in ulcerative colitis
Abstract
Background and aims: Ulcerative colitis disease activity indices offer good statistical power but small changes in these indices may not be clinically important. There are no validated definitions of remission or of significant improvement for these indices. The use of clinically important end points would strengthen the validity of study outcomes. Our aims were to identify objective end points in standard disease activity indices for remission and for improvement in ulcerative colitis.
Methods: Sixty six consecutive patients with ulcerative colitis provided information about remission status and their disease activity. At a return visit 1-14 months later, these patients provided information about the change in their disease activity, and non-invasive indices were measured.
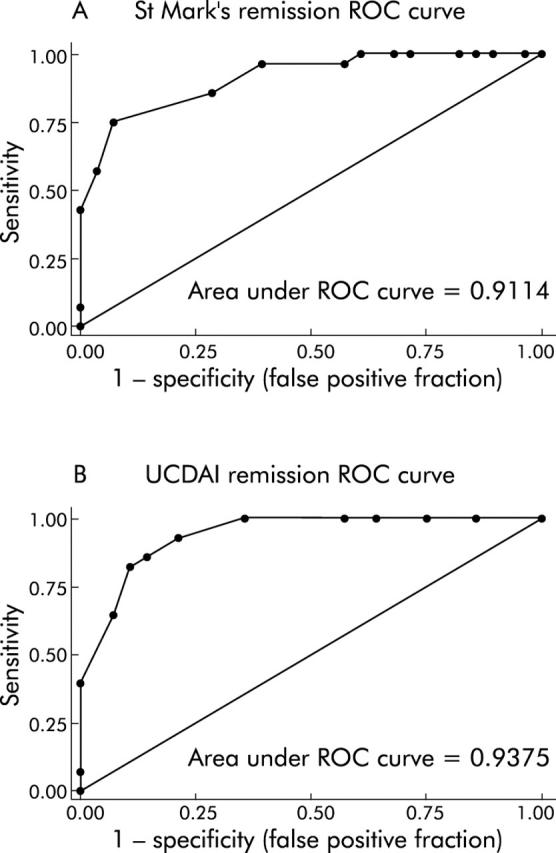
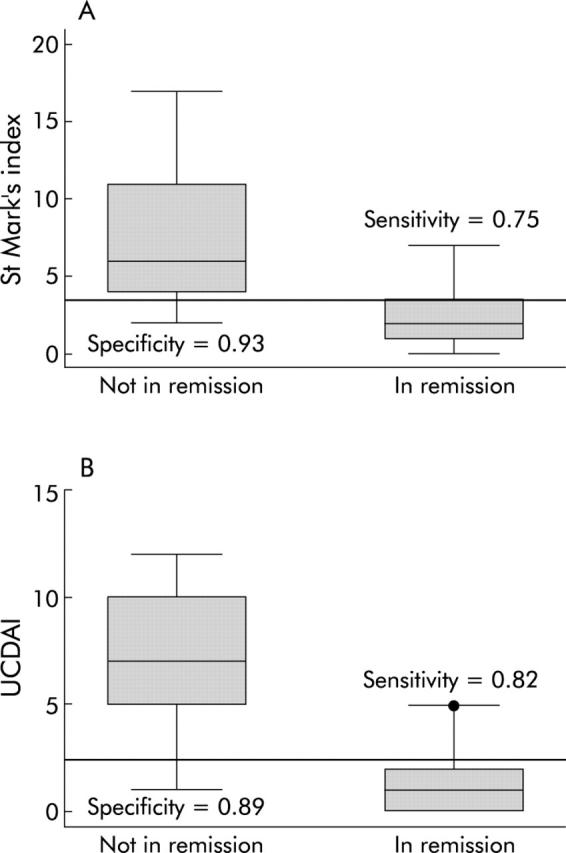
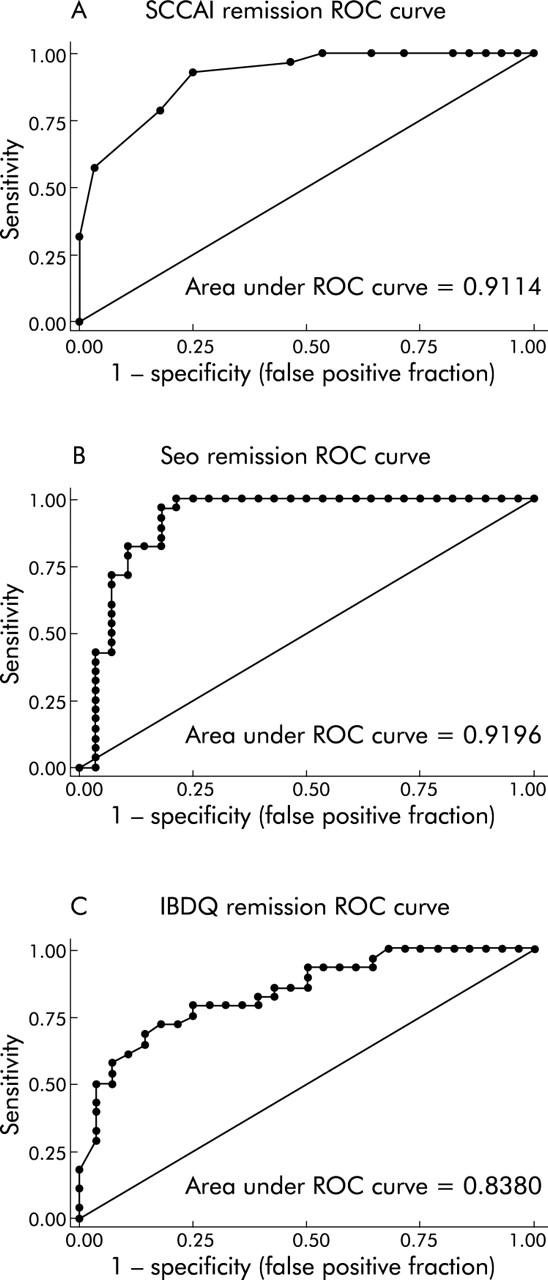
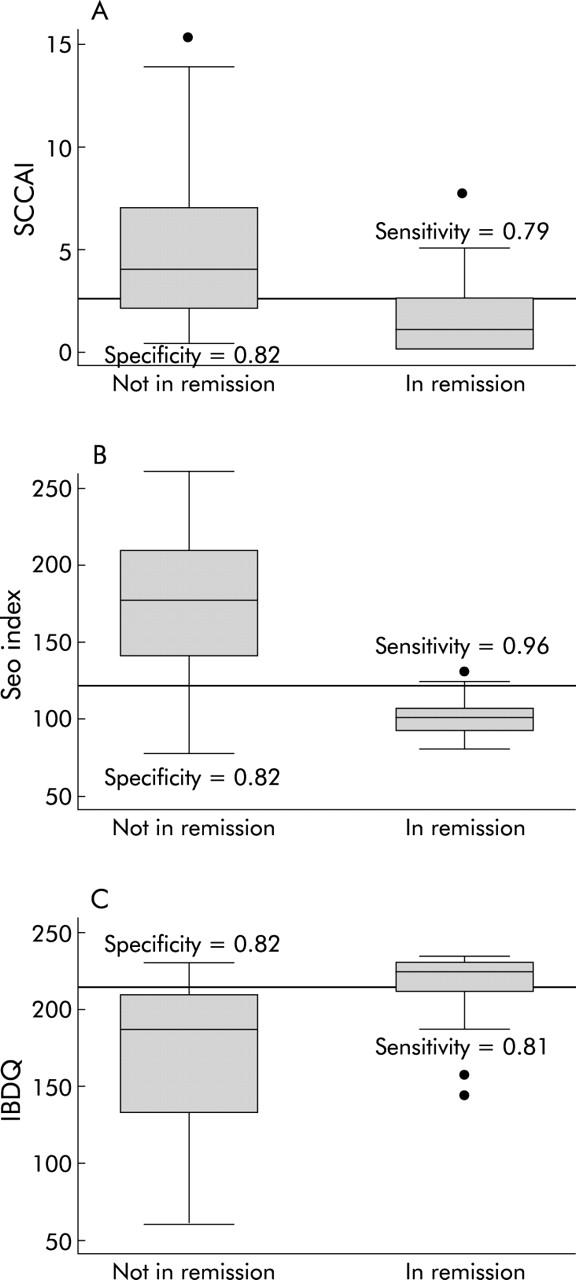
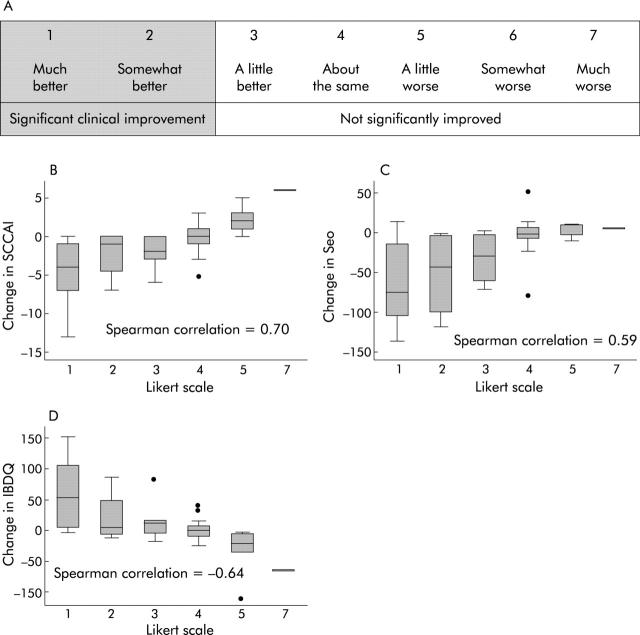
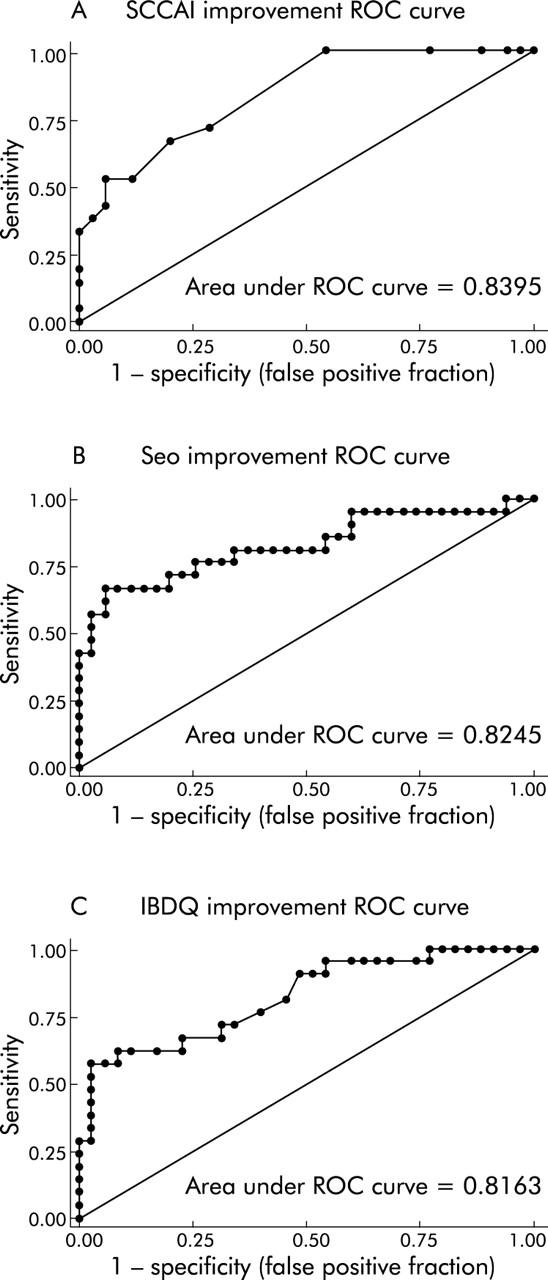
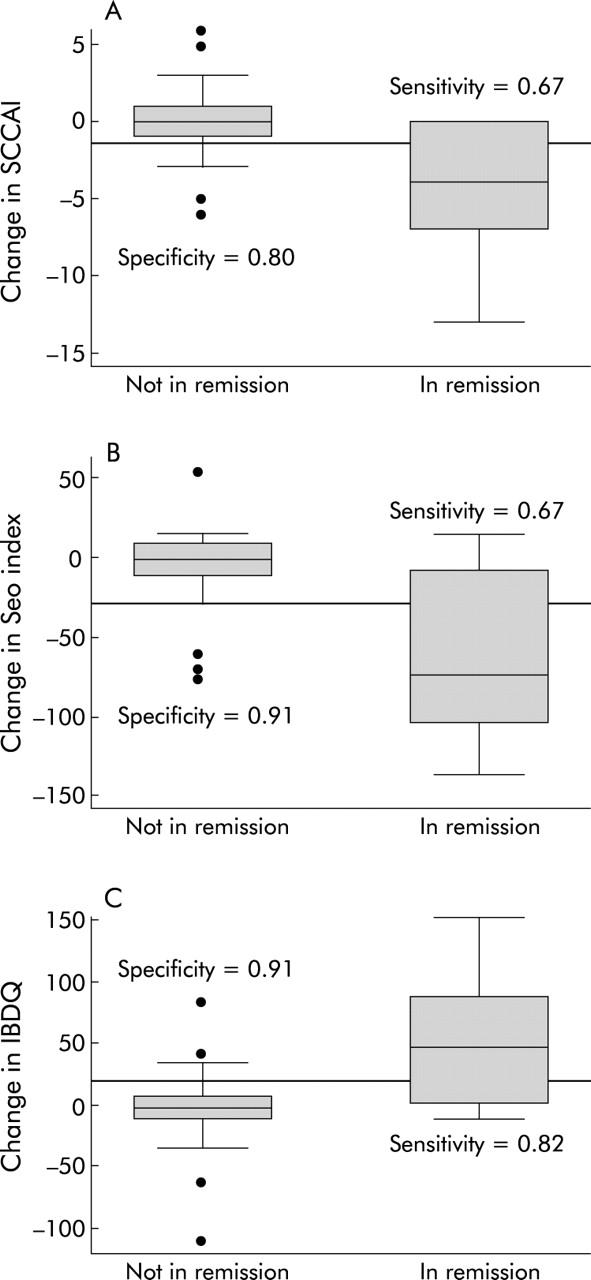
Results: Specific objective end points for determining remission with four standard indices and a quality of life instrument were determined (St Mark's <3.5, ulcerative colitis disease activity index <2.5, simple clinical colitis activity index (SCCAI) <2.5, Seo <120, and inflammatory bowel disease quality of life index (IBDQ) >205). These cut offs also identified patients who met a regulatory definition of remission. Specific objective end points for clinical improvement in two non-invasive indices and a quality of life instrument were determined with good sensitivity and specificity (SCCAI decrease >1.5, Seo decrease >30, IBDQ increase >20).
Conclusions: We found specific cut off values for disease activity indices that identify patients who have significantly improved or achieved remission in an objective, sensitive, and specific manner. These cut offs should help in the interpretation of the outcomes of clinical trials in ulcerative colitis.
Figures
References
-
- Powell-Tuck J, Bown RL, Lennard-Jones JE. A comparison of oral prednisolone given as single or multiple daily doses for active proctocolitis. Scand J Gastroenterol 1978;13:833–7. - PubMed
-
- Sutherland LR, Martin F, Greer S, et al. 5-Aminosalicylic acid enema in the treatment of distal ulcerative colitis, proctosigmoiditis, and proctitis. Gastroenterology 1987;92:1894–8. - PubMed
-
- Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N Engl J Med 1987;317:1625–9. - PubMed
-
- Seo M, Okada M, Yao T, et al. An index of disease activity in patients with ulcerative colitis. Am J Gastroenterol 1992;87:971–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous