

MR imaging of salivary duct carcinoma
- PMID: 15891184
- PMCID: PMC8158590
MR imaging of salivary duct carcinoma
Abstract
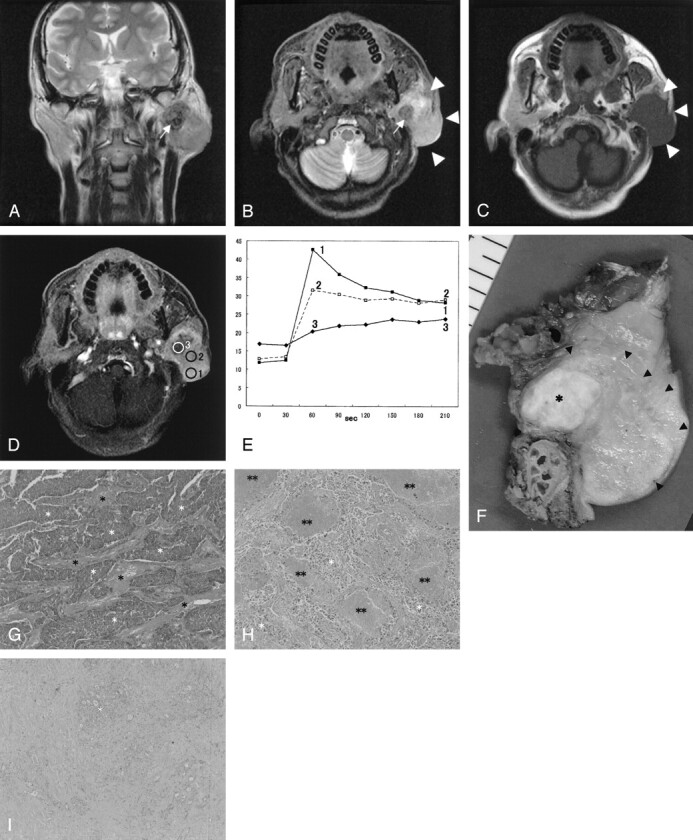
Background and purpose: Salivary duct carcinoma (SDC) is regarded as a high-grade malignancy in the current classification of salivary gland neoplasms. The aim of our study was to describe the MR imaging features of SDC.
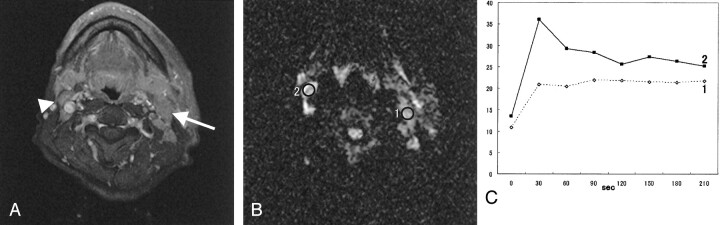
Methods: Nine patients with SDC underwent MR imaging study. The apparent diffusion coefficient (ADC) values of SDCs were measured from diffusion-weighted images. Time-signal intensity curves (TICs) of the tumors on dynamic MR images were plotted, and washout ratios were also calculated. TICs were divided into four types: type A, curve peaks <120 seconds after administration of contrast material with high washout ratio (> or =30%); type B, curve peaks <120 seconds with low washout ratio (<30%); type C, curve peaks >120 seconds; type D, nonenhanced. We correlated the MR findings of SDC with the pathologic findings.
Results: All tumors had ill-defined margins and showed low to moderately high signal intensity for contralateral parotid gland on T2-weighted images. The average of the ADC values of the SDCs was 1.16 +/- 0.14 [SD] x 10(-3)mm(2)/s. Seven of nine (78%) tumors had type B enhancement. On the other hand, six of nine (67%) tumors with rich fibrotic tissue also had type C enhancement.
Conclusion: The findings of ill-defined margin, early enhancement with low washout ratio (type B), and low ADC value (1.22 x 10(-3)mm(2)/s) were useful for suggesting malignant salivary gland tumors. Although it was reported that type C enhancement was specific for pleomorphic adenoma, SDC frequently has type C-enhanced focus.
Figures
References
-
- Kleinsasser O, Klein HJ, Hubner G. Speichelgangcarcinomas: Ein den Milchgangcarcinomen der Brustdruse Analoge Gruppe von Speicheldrusentumoren. Arch Klin Exp Ohren Nasen Kehlkopfheikd 1968;192:100–105 - PubMed
-
- Seifert G, Sobin LH. Histological Typing of Salivary Gland Tumors: World Health Organization International Histological Classification of tumors. 2nd ed. New York: Springer-Verlag;1991
-
- Yabuuchi H, Fukuya T, Tajima T, et al. Salivary gland tumors: diagnostic value of gadolinium-enhanced dynamic MR imaging with histopathologic correlation. Radiology 2003;226:345–354 - PubMed
-
- Chen KT, Hafez GR. Infiltrating salivary duct carcinoma: a clinicopathologic study of five cases. Arch Otolaryngol 1981;107:37–39 - PubMed
-
- Chen KT. Intraductal carcinoma of the minor salivary gland. J Laryngol Otol 1983;97:189–191 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical