

Efficacy of treatment of severe carotid bifurcation stenosis by using self-expanding stents without deliberate use of angioplasty balloons
- PMID: 15891192
- PMCID: PMC8158633
Efficacy of treatment of severe carotid bifurcation stenosis by using self-expanding stents without deliberate use of angioplasty balloons
Abstract
Background and purpose: One of the limitations of carotid artery angioplasty is the potential for embolic stroke. Our purpose was to assess whether the force of a self-expanding stent alone is usually sufficient to dilate severely stenotic atherosclerotic plaques without the deliberate use of an angioplasty balloon. If so, the procedural stroke risk might be reduced.
Methods: Over a 30-month period, 21 consecutive patients were prospectively identified with severe symptomatic carotid artery stenosis (>70% NASCET [North American Symptomatic Carotid Endarterectomy Trial]) and relative indications for endovascular treatment. All underwent treatment with the aim of deploying a self-expanding stent across the stenosis without the use of angioplasty balloons or distal protection devices.
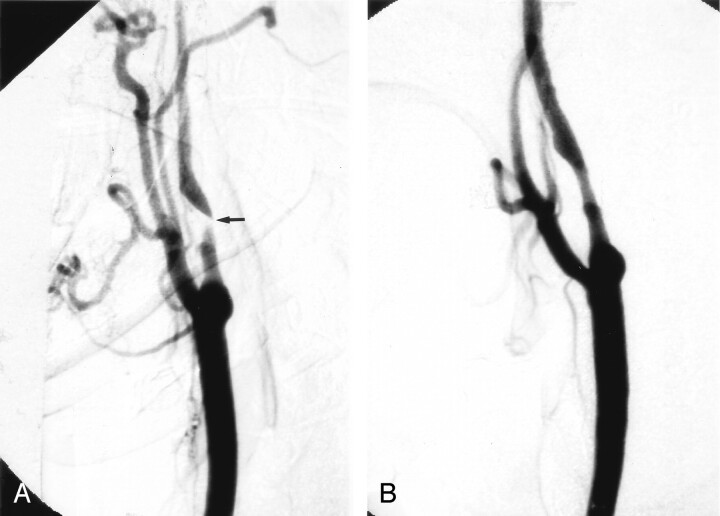
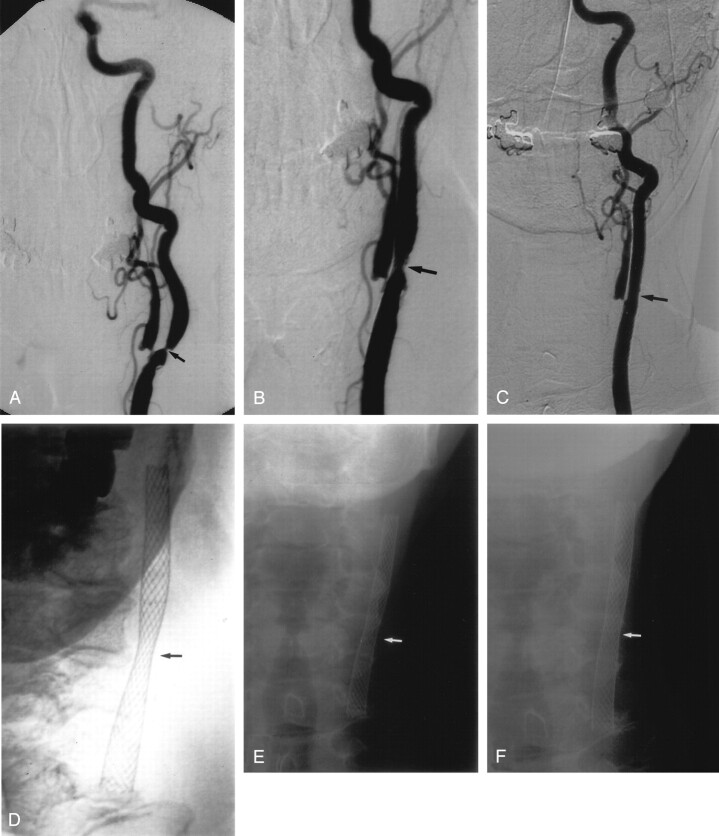
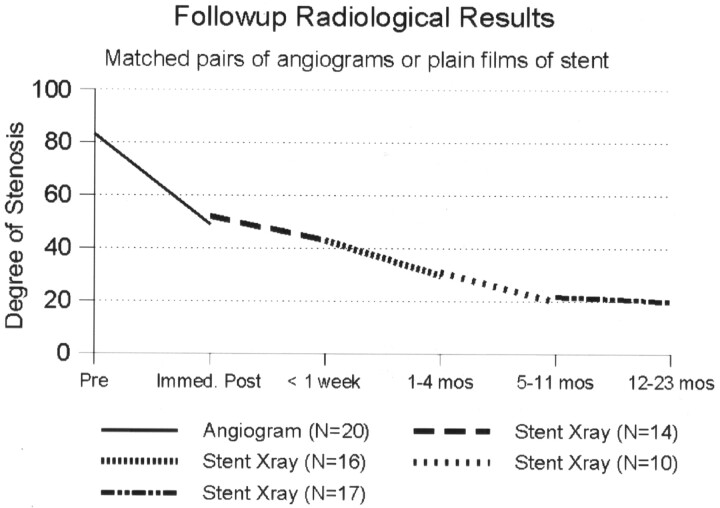
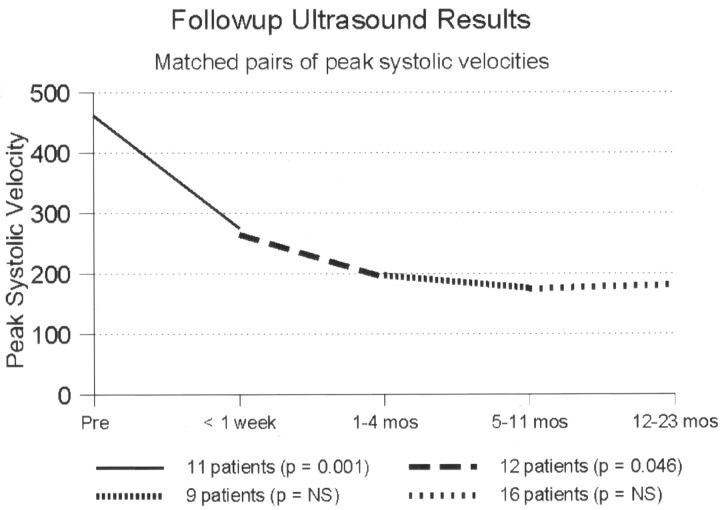
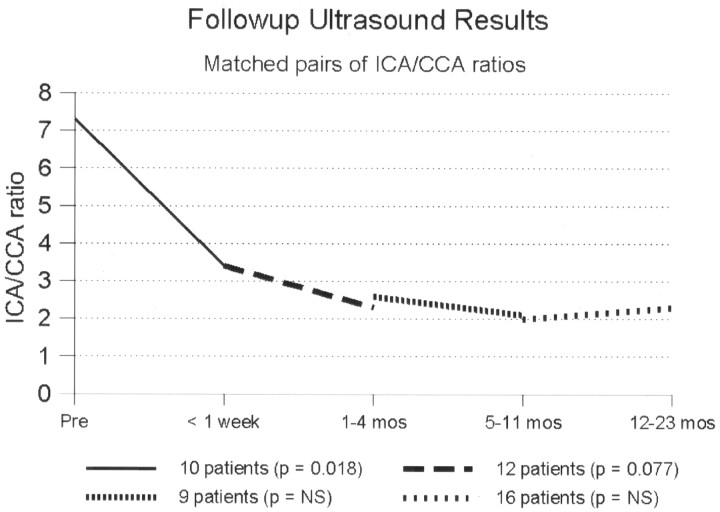
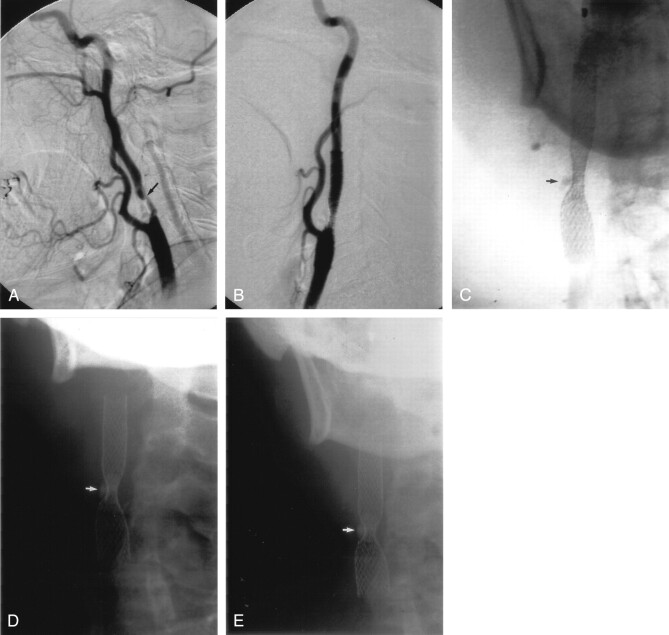
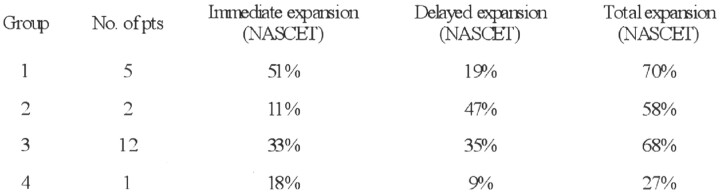
Results: Stent deployment was successful in 20/21 patients. In one patient, the stent could not be deployed without balloon predilatation and a stroke occurred. In the other 20 patients, angiography before and immediately after stent deployment showed a reduction in the mean stenosis from 83% to 49%. A second periprocedural stroke occurred as a result of early stent thrombosis at 4 days in a patient who stopped Acetylsalicylic acid while undergoing bowel preparation for colon surgery. He made a good recovery. Average duration of follow-up imaging was 19 months (range, 1-44 months). During the follow-up period there were four deaths, all unrelated to the carotid disease, and no major strokes. At 5-11 months, the average residual stenosis was 21%, which remained stable in 16 of the 18 patients studied between 12 and 44 months (average, 24 months). At last follow-up, in these 16 the mean peak systolic velocity was 123 cm/s (range, 60-238 cm/s) and the mean internal-to-common carotid ratio was 1.8. The other two patients were long-term failures of the "stent-only" approach. In one patient, a heavily calcified plaque prevented stent expansion and the artery occluded at 18 months with a minor stroke. In the second patient, a recurrent stenosis developed at 16 months with one episode of transient ischemic attack.
Conclusion: Deployment of a self-expanding stent alone resulted in a favorable and more gradual reduction of severe symptomatic carotid stenosis. Improvements in stent profile and chronic outward force may widen the indications for simple stent placement without the use of balloons or adjunctive protection devices.
Figures
Similar articles
-
Results using a self-expanding stent alone in the treatment of severe symptomatic carotid bifurcation stenosis.J Neurosurg. 2008 Sep;109(3):454-60. doi: 10.3171/JNS/2008/109/9/0454. J Neurosurg. 2008. PMID: 18759576
-
Safety of latest-generation self-expanding stents in patients with NASCET-ineligible severe symptomatic extracranial internal carotid artery stenosis.Arch Neurol. 2004 Jan;61(1):39-43. doi: 10.1001/archneur.61.1.39. Arch Neurol. 2004. PMID: 14732618
-
Plaque morphology (the PLAC Scale) on CT angiography: predicting long-term anatomical success of primary carotid stenting.J Neurosurg. 2015 Oct;123(4):856-61. doi: 10.3171/2014.9.JNS14811. Epub 2015 Mar 27. J Neurosurg. 2015. PMID: 25816084
-
Balloon Angioplasty for In-Stent Restenosis Resulting in Carotid Stent Fracture: Literature Review of Stent-in-Stent Technique as a Viable Therapeutic Option.World Neurosurg. 2017 May;101:818.e1-818.e6. doi: 10.1016/j.wneu.2017.01.127. Epub 2017 Feb 10. World Neurosurg. 2017. PMID: 28192264 Review.
-
Will mesh-covered stents help reduce stroke associated with carotid stent angioplasty?Semin Vasc Surg. 2017 Mar;30(1):25-30. doi: 10.1053/j.semvascsurg.2017.04.007. Epub 2017 Apr 27. Semin Vasc Surg. 2017. PMID: 28818256 Review.
Cited by
-
Novel 3D-CT evaluation of carotid stent volume: greater chronological expansion of stents in patients with vulnerable plaques.Neuroradiology. 2013 Sep;55(9):1153-60. doi: 10.1007/s00234-013-1223-0. Epub 2013 Jul 3. Neuroradiology. 2013. PMID: 23821124 Clinical Trial.
-
Carotid stenting without use of balloon angioplasty and distal protection devices: preliminary experience in 100 cases.AJNR Am J Neuroradiol. 2007 Aug;28(7):1378-83. doi: 10.3174/ajnr.A0543. AJNR Am J Neuroradiol. 2007. PMID: 17698546 Free PMC article.
-
Locking between a cerebral protection device and a stent-delivering catheter during carotid artery stenting.Interv Neuroradiol. 2014 Jan-Feb;20(1):100-5. doi: 10.15274/INR-2014-10015. Epub 2014 Feb 10. Interv Neuroradiol. 2014. PMID: 24556307 Free PMC article.
-
Carotid angioplasty and stenting without protection devices: safety and efficacy concerns--single center experience.Clin Neuroradiol. 2011 Jun;21(2):65-73. doi: 10.1007/s00062-011-0057-6. Epub 2011 May 12. Clin Neuroradiol. 2011. PMID: 21562830
-
Letter - Re: Primary carotid stenting without angioplasty.Interv Neuroradiol. 2008 Dec 29;14(4):473. Epub 2009 Jan 5. Interv Neuroradiol. 2008. PMID: 20557751 Free PMC article. No abstract available.
References
-
- Phatouros CC, Higashida RT, Malek AM, et al. Carotid artery stent placement for atherosclerotic disease: rationale, technique, and current status. Radiology 2000;217:26–41 - PubMed
-
- Wholey MH, Wholey M, Bergeron P, et al. Current global status of carotid artery stent placement. Cathet Cardiovasc Diagn 1998;44:1– 6 - PubMed
-
- Roubin GS, Yadav S, Iyer SS, Vitek J. Carotid stent supported angioplasty: a neurovascular intervention to prevent stroke. Am J Cardiol 1996;78:8– 12 - PubMed
-
- Carotid and Vertebral Artery Transluminal Angioplasty Study. Endovascular versus surgical treatment in patients with carotid stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): a randomised trial. Lancet 2001;357:1729– 1737 - PubMed
-
- Martin JB, Pache JC, Treggiari-Venzi M, et al. Role of the distal balloon protection technique in the prevention of cerebral embolic events during carotid stent placement. Stroke 2001;32:479– 484 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources