

Psychological illness is commonly associated with functional gastrointestinal disorders and is important to consider during patient consultation: a population-based study
- PMID: 15892883
- PMCID: PMC1156899
- DOI: 10.1186/1741-7015-3-8
Psychological illness is commonly associated with functional gastrointestinal disorders and is important to consider during patient consultation: a population-based study
Abstract
Background: Some individuals with functional gastrointestinal disorders (FGID) suffer long-lasting symptoms without ever consulting their doctors. Our aim was to study co-morbidity and lifestyle differences among consulters and non-consulters with persistent FGID and controls in a defined adult population.
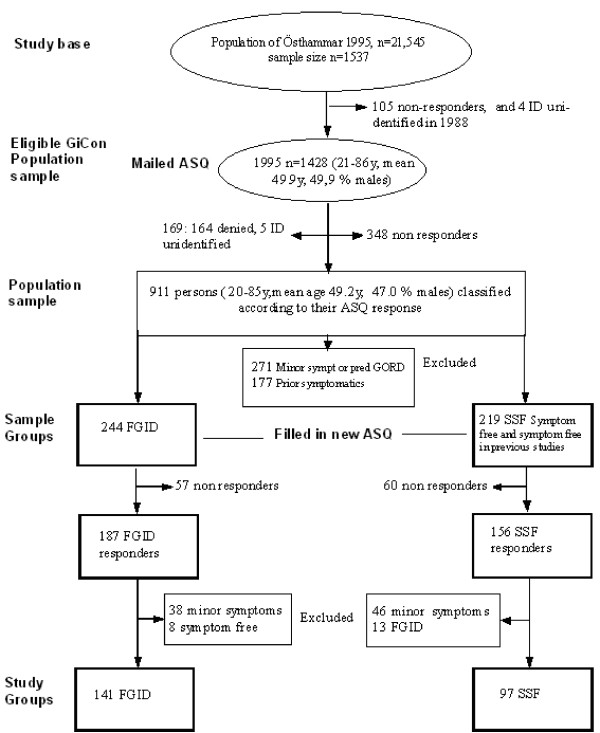
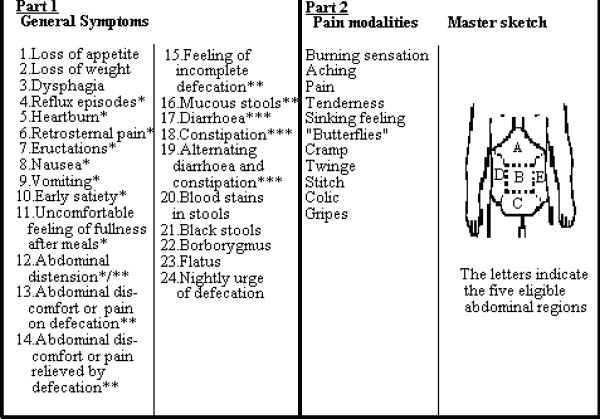
Methods: A random sample of the general adult Swedish population was obtained by a postal questionnaire. The Abdominal Symptom Questionnaire (ASQ) was used to measure GI symptomatology and grade of GI symptom severity and the Complaint Score Questionnaire (CSQ) was used to measure general symptoms. Subjects were then grouped for study by their symptomatic profiles. Subjects with long-standing FGID (n = 141) and subjects strictly free from gastrointestinal (GI) symptoms (n = 97) were invited to attend their local health centers for further assessment.
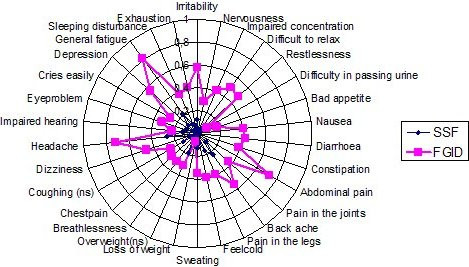
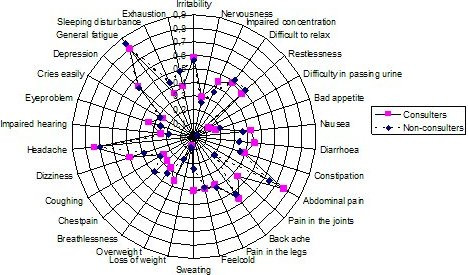
Results: Subjects with FGID have a higher risk of psychological illness [OR 8.4, CI95(4.0-17.5)] than somatic illness [OR 2.8, CI95(1.3-5.7)] or ache and fatigue symptoms [OR 4.3, CI95(2.1-8.7)]. Subjects with psychological illness have a higher risk of severe GI symptoms than controls; moreover they have a greater chance of being consulters. Patients with FGID have more severe GI symptoms than non-patients.
Conclusion: There is a strong relation between extra-intestinal, mental and somatic complaints and FGID in both patients and non-patients. Psychological illness increases the chance of concomitantly having more severe GI symptoms, which also enhance consultation behaviour.
Figures
References
-
- Talley NJ, Zinsmeister AR, Schleck CD, Melton LJ., III Dyspepsia and dyspepsia subgroups: a population-based study. Gastroenterology. 1992;102:1259–68. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
