

CDX1 is an important molecular mediator of Barrett's metaplasia
- PMID: 15894614
- PMCID: PMC1140438
- DOI: 10.1073/pnas.0502031102
CDX1 is an important molecular mediator of Barrett's metaplasia
Abstract
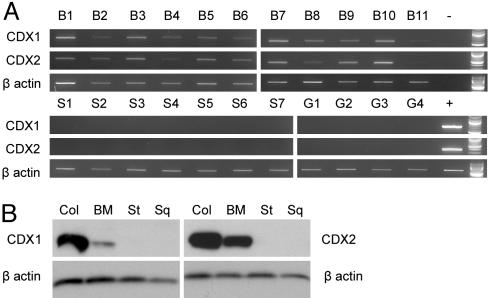
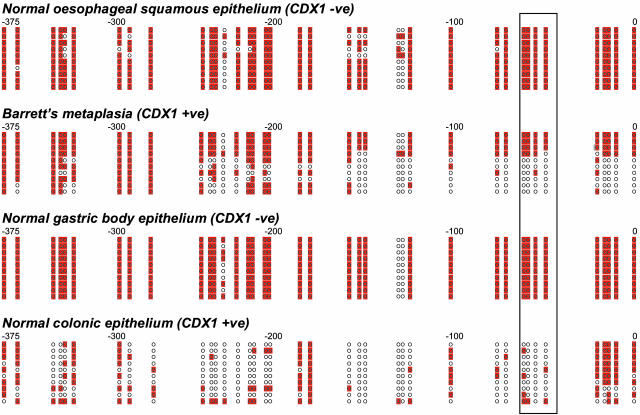
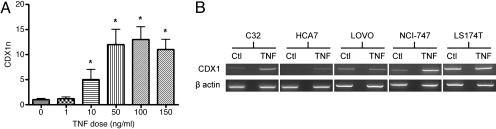
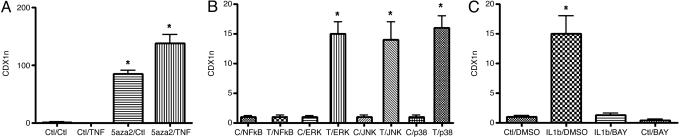
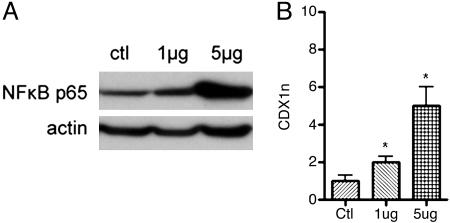
The molecular pathogenesis of Barrett's metaplasia (BM) of the esophagus is poorly understood. The change to an intestinal phenotype occurs on a background of esophagitis due to refluxing acid and bile. CDX1, an important regulator of normal intestinal development, was studied as a potential key molecule in the pathogenesis of BM. CDX1 mRNA and protein were universally expressed in all samples of BM tested but not in normal esophageal squamous or gastric body epithelia. This tissue-specific expression was attributable to the methylation status of the CDX1 promoter. Conjugated bile salts and the inflammatory cytokines TNF-alpha and IL-1beta were all found to increase CDX1 mRNA expression in vitro. These effects were primarily mediated by NF-kappaB signaling but only occurred when the CDX1 promoter was unmethylated or partially methylated. The data suggest that CDX1 is a key molecule linking etiological agents of BM to the development of an intestinal phenotype. Although the initial trigger for CDX1 promoter demethylation is not yet identified, it seems likely that demethylation of its promoter may be the key to the induction and maintenance of CDX1 expression and so of the BM phenotype.
Figures

References
-
- Nandurkar, S. & Talley, N. J. (1999) Am. J. Gastroenterol. 94, 30–40. - PubMed
-
- Wild, C. P. & Hardie, L. J. (2003) Nat. Rev. Cancer 3, 676–684. - PubMed
-
- Freund, J. N., Domon-Dell, C., Kedinger, M. & Duluc, I. (1998) Biochem. Cell Biol. 76, 957–969. - PubMed
-
- Eda, A., Osawa, H., Yanaka, I., Satoh, K., Mutoh, H., Kihira, K. & Sugano, K. (2002) J. Gastroenterol. 37, 94–100. - PubMed
-
- Eda, A., Osawa, H., Satoh, K., Yanaka, I., Kihira, K., Ishino, Y., Mutoh, H. & Sugano, K. (2003) J. Gastroenterol. 38, 14–22. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
