

Effect of prone position on regional shunt, aeration, and perfusion in experimental acute lung injury
- PMID: 15901611
- PMCID: PMC2718529
- DOI: 10.1164/rccm.200501-004OC
Effect of prone position on regional shunt, aeration, and perfusion in experimental acute lung injury
Abstract
Rationale: The prone position is used to improve gas exchange in patients with acute respiratory distress syndrome. However, the regional mechanism by which the prone position improves gas exchange in acutely injured lungs is still incompletely defined.
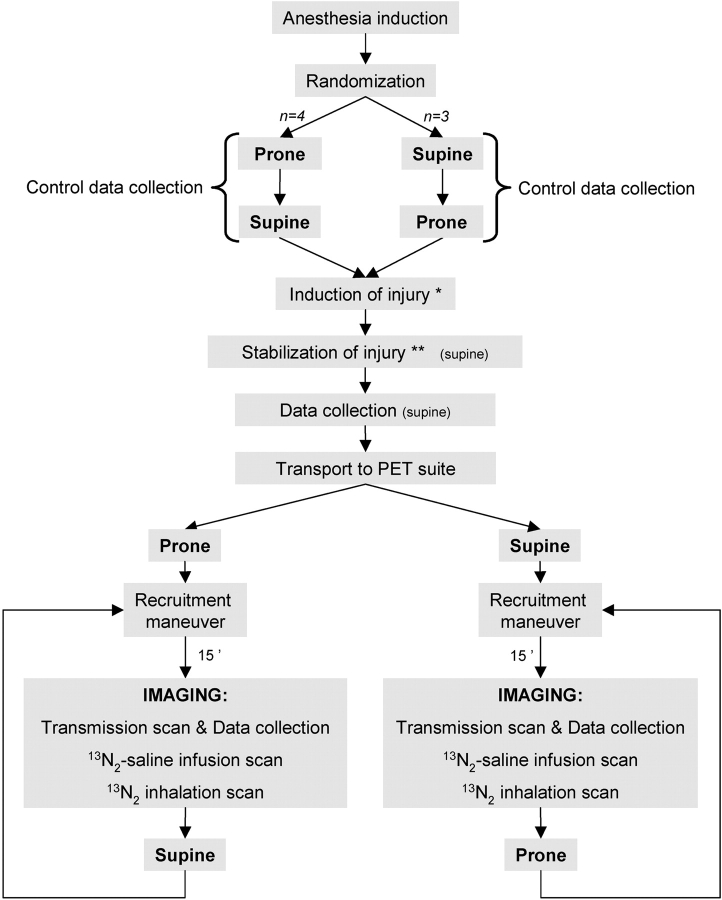
Methods: We used positron emission tomography imaging of [(13)N]nitrogen to assess the regional distribution of pulmonary shunt, aeration, perfusion, and ventilation in seven surfactant-depleted sheep in supine and prone positions.
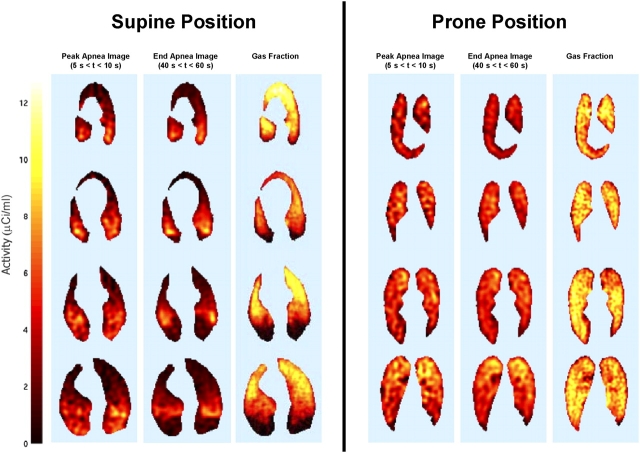
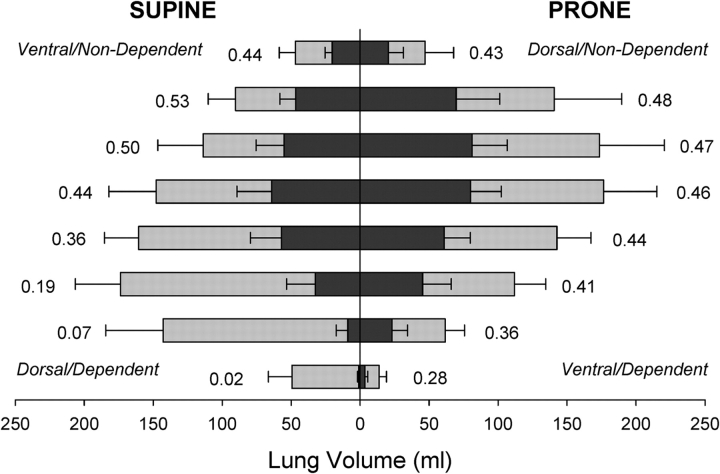
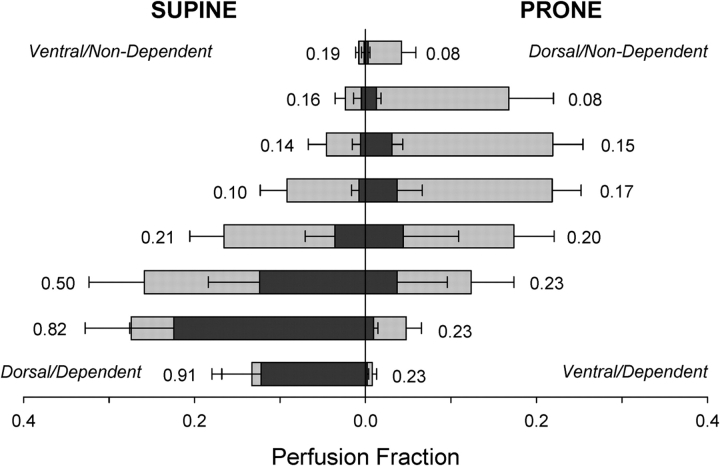
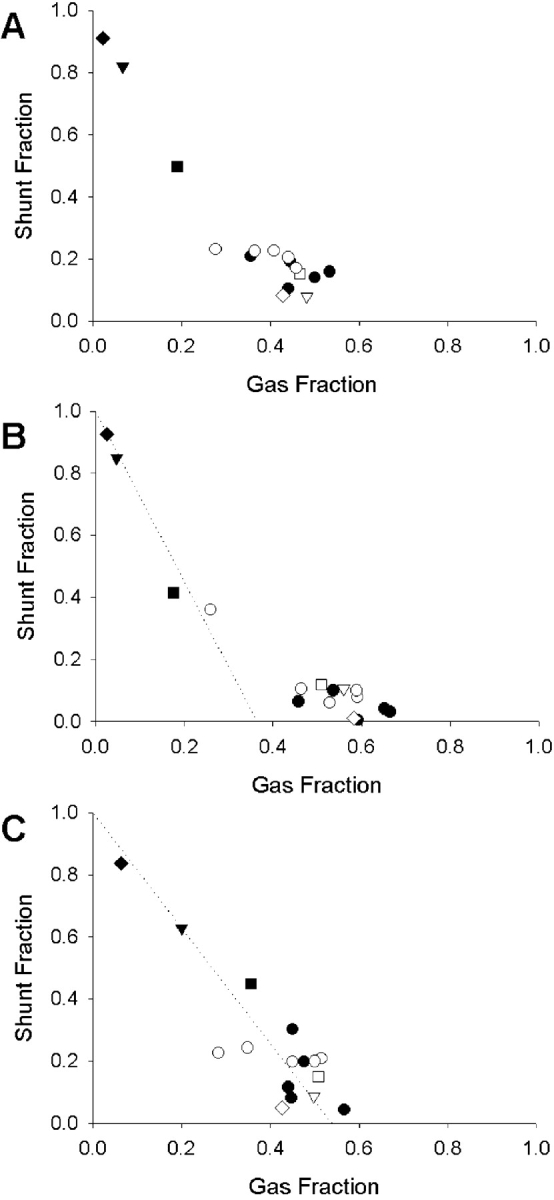
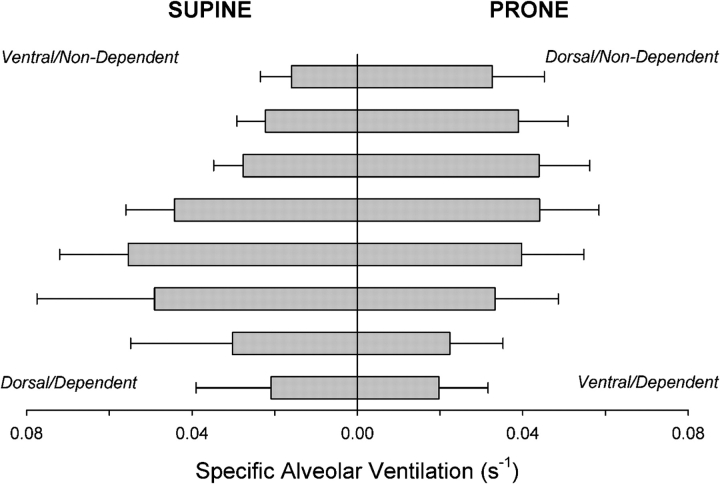
Results: In the supine position, the dorsal lung regions had a high shunt fraction, high perfusion, and poor aeration. The prone position was associated with an increase in lung gas content and with a more uniform distribution of aeration, as the increase in aeration in dorsal lung regions was not offset by loss of aeration in ventral regions. Consequently, the shunt fraction decreased in dorsal regions in the prone position without a concomitant impairment of gas exchange in ventral regions, thus leading to a significant increase in the fraction of pulmonary perfusion participating in gas exchange. In addition, the vertical distribution of specific alveolar ventilation became more uniform in the prone position. A biphasic relation between regional shunt fraction and gas fraction showed low shunt for values of gas fraction higher than a threshold, and a steep linear increase in shunt for lower values of gas fraction.
Conclusion: In a surfactant-deficient model of lung injury, the prone position improved gas exchange by restoring aeration and decreasing shunt while preserving perfusion in dorsal lung regions, and by making the distribution of ventilation more uniform.
Figures
Similar articles
-
Mechanism by which the prone position improves oxygenation in acute lung injury.Am J Respir Crit Care Med. 1994 Jul;150(1):184-93. doi: 10.1164/ajrccm.150.1.8025748. Am J Respir Crit Care Med. 1994. PMID: 8025748
-
Marked differences between prone and supine sheep in effect of PEEP on perfusion distribution in zone II lung.J Appl Physiol (1985). 2005 Sep;99(3):909-14. doi: 10.1152/japplphysiol.01388.2004. Epub 2005 Mar 17. J Appl Physiol (1985). 2005. PMID: 15774701
-
Effects of prone position and positive end-expiratory pressure on lung perfusion and ventilation.Crit Care Med. 2008 Aug;36(8):2373-80. doi: 10.1097/CCM.0b013e31818094a9. Crit Care Med. 2008. PMID: 18596639
-
Prone position improves gas exchange--but how?Acta Anaesthesiol Scand. 2001 Feb;45(2):150-9. Acta Anaesthesiol Scand. 2001. PMID: 11167159 Review.
-
Gas Exchange in the Prone Posture.Respir Care. 2017 Aug;62(8):1097-1110. doi: 10.4187/respcare.05512. Epub 2017 May 30. Respir Care. 2017. PMID: 28559471 Review.
Cited by
-
Translational Role of Rodent Models to Study Ventilator-Induced Lung Injury.Transl Perioper Pain Med. 2021 Dec;8(4):404-415. Epub 2021 Nov 27. Transl Perioper Pain Med. 2021. PMID: 34993270 Free PMC article.
-
Therapeutic benefits of proning to improve pulmonary gas exchange in severe respiratory failure: focus on fundamentals of physiology.Exp Physiol. 2022 Jul;107(7):759-770. doi: 10.1113/EP089405. Epub 2021 Aug 13. Exp Physiol. 2022. PMID: 34242438 Free PMC article. Review.
-
Mechanisms of the effects of prone positioning in acute respiratory distress syndrome.Intensive Care Med. 2014 Nov;40(11):1634-42. doi: 10.1007/s00134-014-3500-8. Epub 2014 Sep 30. Intensive Care Med. 2014. PMID: 25266133 Review.
-
Positional Therapy and Regional Pulmonary Ventilation.Anesthesiology. 2020 Nov 1;133(5):1093-1105. doi: 10.1097/ALN.0000000000003509. Anesthesiology. 2020. PMID: 32773690 Free PMC article.
-
Spatial-temporal dynamics of pulmonary blood flow in the healthy human lung in response to altered FI(O2).J Appl Physiol (1985). 2013 Jan 1;114(1):107-18. doi: 10.1152/japplphysiol.00433.2012. Epub 2012 Oct 25. J Appl Physiol (1985). 2013. PMID: 23104691 Free PMC article.
References
-
- Gattinoni L, Tognoni G, Pesenti A, Taccone P, Mascheroni D, Labarta V, Malacrida R, Di Giulio P, Fumagalli R, Pelosi P, et al. Effect of prone positioning on the survival of patients with acute respiratory failure. N Engl J Med 2001;345:568–573. - PubMed
-
- Papazian L, Bregeon F, Gaillat F, Thirion X, Gainnier M, Gregoire R, Saux P, Gouin F, Jammes Y, Auffray JP. Respective and combined effects of prone position and inhaled nitric oxide in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med 1998;157:580–585. - PubMed
-
- Wiener CM, Kirk W, Albert RK. Prone position reverses gravitational distribution of perfusion in dog lungs with oleic acid-induced lung injury. J Appl Physiol 1990;68:1386–1392. - PubMed
-
- Lamm WJ, Graham MM, Albert RK. Mechanism by which the prone position improves oxygenation in acute lung injury. Am J Respir Crit Care Med 1994;150:184–193. - PubMed
-
- Gattinoni L, Vagginelli F, Carlesso E, Taccone P, Conte V, Chiumello D, Valenza F, Caironi P, Pesenti A. Decrease in PaCO2 with prone position is predictive of improved outcome in acute respiratory distress syndrome. Crit Care Med 2003;31:2727–2733. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
