

Effectiveness of highly active antiretroviral therapy among injection drug users with late-stage human immunodeficiency virus infection
- PMID: 15901620
- PMCID: PMC4078731
- DOI: 10.1093/aje/kwi133
Effectiveness of highly active antiretroviral therapy among injection drug users with late-stage human immunodeficiency virus infection
Abstract
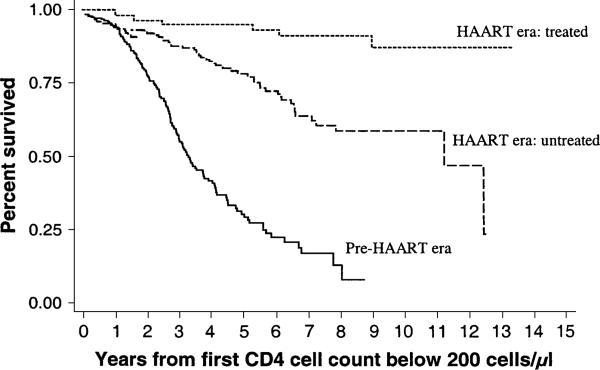
Highly active antiretroviral therapy (HAART) has been shown to be effective in different populations, but data among injection drug users are limited. Human immunodeficiency virus-infected injection drug users recruited into the Acquired Immunodeficiency Syndrome Link to Intravenous Experiences (ALIVE) Study as early as 1988 were tested semiannually to identify their first CD4-positive T-lymphocyte cell count below 200/microl; they were followed for mortality through 2002. Visits were categorized into the pre-HAART (before mid-1996) and the HAART eras and further categorized by HAART use. Survival analysis with staggered entry was used to evaluate the effect of HAART on acquired immunodeficiency syndrome-related mortality, adjusting for other medications and demographic, clinical, and behavioral factors. Among 665 participants, 258 died during 2,402 person-years of follow-up. Compared with survival in the pre-HAART era, survival in the HAART era was shown by multivariate analysis to be improved for both those who did and did not receive HAART (relative hazards = 0.06 and 0.33, respectively; p < 0.001). Inferences were unchanged after restricting analyses to data starting with 1993 and considerations of lead-time bias and human immunodeficiency viral load. The annual CD4-positive T-lymphocyte cell decline was less in untreated HAART-era participants than in pre-HAART-era participants (-10/microl vs. -37/microl, respectively), suggesting that changing indications for treatment may have contributed to improved survival and that analyses restricted to the HAART era probably underestimate HAART effectiveness.
Figures
References
-
- Hammer SM, Squires KE, Hughes MD, et al. A controlled trial of two nucleoside analogues plus indinavir in persons with human immunodeficiency virus infection and CD4 cell counts of 200 per cubic millimeter or less. AIDS Clinical Trials Group 320 Study Team. N Engl J Med. 1997;337:725–33. - PubMed
-
- Detels R, Munoz A, McFarlane G, et al. Effectiveness of potent antiretroviral therapy on time to AIDS and death in men with known HIV infection duration. Multicenter AIDS Cohort Study Investigators. JAMA. 1998;280:1497–503. - PubMed
-
- Survival after introduction of HAART in people with known duration of HIV-1 infection. The CASCADE Collaboration. Concerted Action on SeroConversion to AIDS and Death in Europe. Lancet. 2000;355:1158–9. - PubMed
-
- Murphy EL, Collier AC, Kalish LA, et al. Highly active antiretroviral therapy decreases mortality and morbidity in patients with advanced HIV disease. Ann Intern Med. 2001;135:17–26. - PubMed
-
- Anastos K, Barron Y, Miotti P, et al. Risk of progression to AIDS and death in women infected with HIV-1 initiating highly active antiretroviral treatment at different stages of disease. Arch Intern Med. 2002;162:1973–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
