

Progestins and progesterone in hormone replacement therapy and the risk of breast cancer
- PMID: 15908197
- PMCID: PMC1974841
- DOI: 10.1016/j.jsbmb.2005.02.014
Progestins and progesterone in hormone replacement therapy and the risk of breast cancer
Abstract
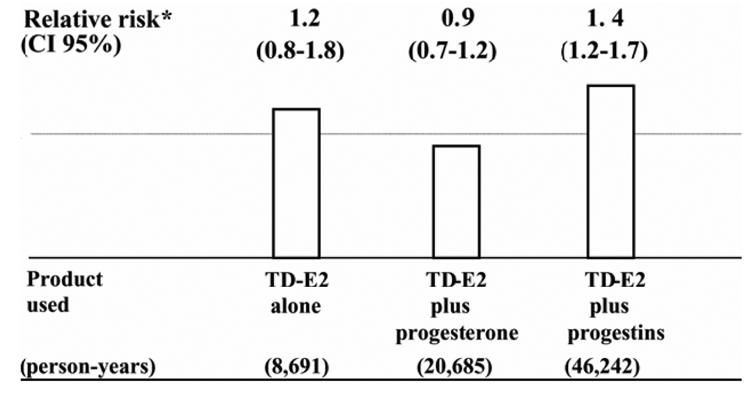
Controlled studies and most observational studies published over the last 5 years suggest that the addition of synthetic progestins to estrogen in hormone replacement therapy (HRT), particularly in continuous-combined regimen, increases the breast cancer (BC) risk compared to estrogen alone. By contrast, a recent study suggests that the addition of natural progesterone in cyclic regimens does not affect BC risk. This finding is consistent with in vivo data suggesting that progesterone does not have a detrimental effect on breast tissue. The increased BC risk found with the addition of synthetic progestins to estrogen could be due to the regimen and/or the kind of progestin used. Continuous-combined regimen inhibits the sloughing of mammary epithelium that occurs after progesterone withdrawal in a cyclic regimen. More importantly, the progestins used (medroxyprogesterone acetate and 19-Nortestosterone-derivatives) are endowed with some non-progesterone-like effects, which can potentiate the proliferative action of estrogens. Particularly relevant seem to be the metabolic and hepatocellular effects (decreased insulin sensitivity, increased levels and activity of insulin-like growth factor-I, and decreased levels of SHBG), which contrast the opposite effects induced by oral estrogen.
Figures


 ) mainly medroxyprogesterone acetate (MPA); (
) mainly medroxyprogesterone acetate (MPA); (
 ) 19-Nortestosterone-derived progestins and (20%) MPA; (*) only 19-Nortestosterone-derived progestins; (▴) mainly 19-Nortestosterone-derived progestins.
) 19-Nortestosterone-derived progestins and (20%) MPA; (*) only 19-Nortestosterone-derived progestins; (▴) mainly 19-Nortestosterone-derived progestins.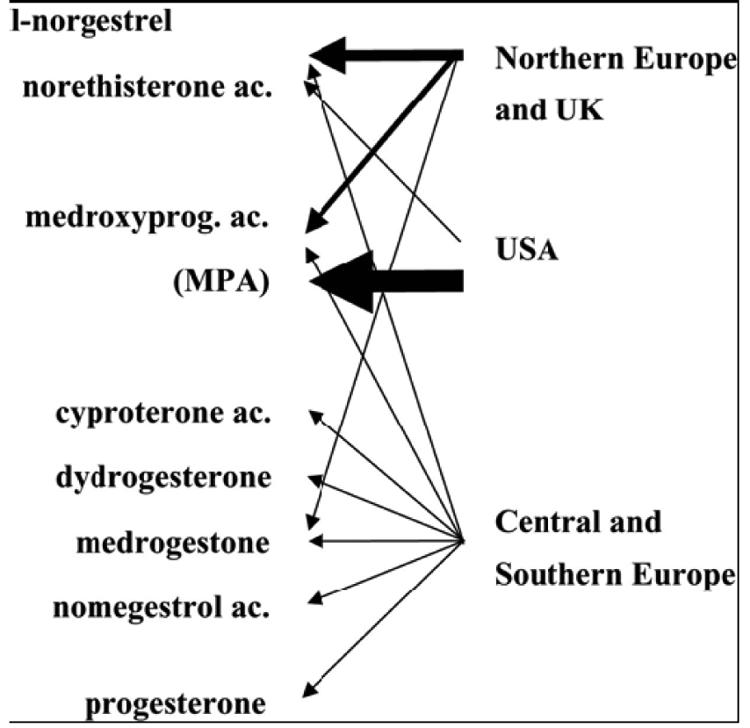
References
-
- Clemmesen J. Statistical studies in the aetiology of malignant neoplasms, 3. Acta Pathol Microbiol Scand. 1969;209(S1):S1–S58. - PubMed
-
- Trichopoulos D, MacMahon B, Cole P. Menopause and breast cancer risk. J Natl Cancer Inst. 1972;48(3):605–613. - PubMed
-
- Early Breast Cancer Trialists’ Collaborative Group. Tamoxifen for early breast cancer: an overview of the randomised trials. Lancet. 1998;351(9114):1451–1467. - PubMed
-
- Endogenous sex hormones and breast cancer in postmenopausal women: reanalysis of nine prospective studies. J Natl Cancer Inst. 2002;94(8):606–616. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
