

Electromechanical analysis of infarct border zone in chronic myocardial infarction
- PMID: 15908463
- PMCID: PMC2396317
- DOI: 10.1152/ajpheart.00423.2005
Electromechanical analysis of infarct border zone in chronic myocardial infarction
Abstract
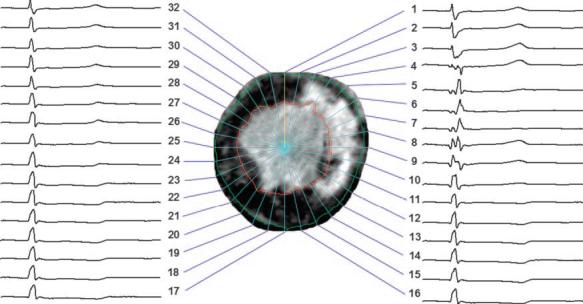
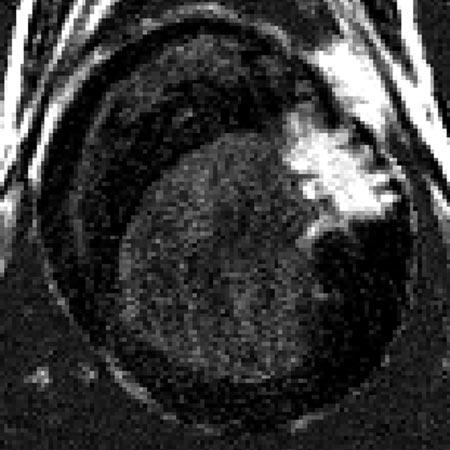
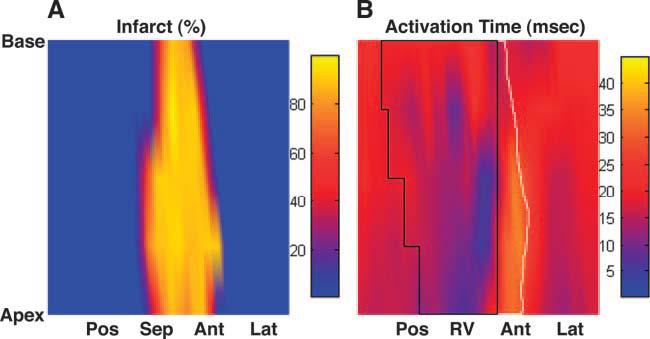
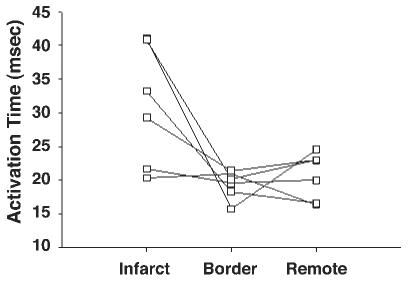
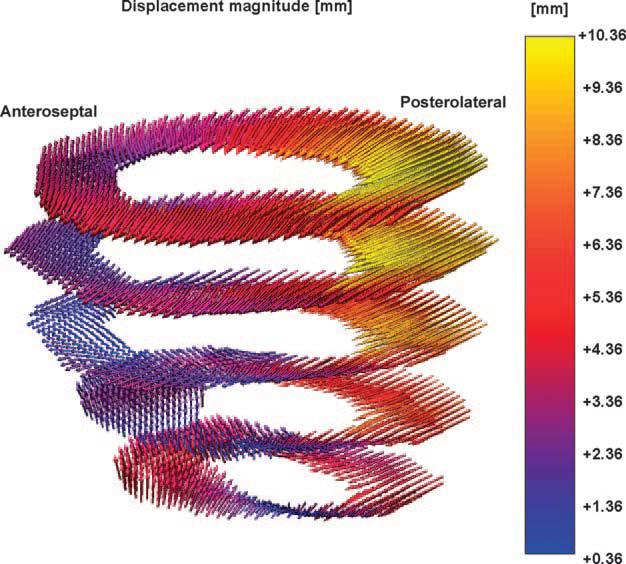
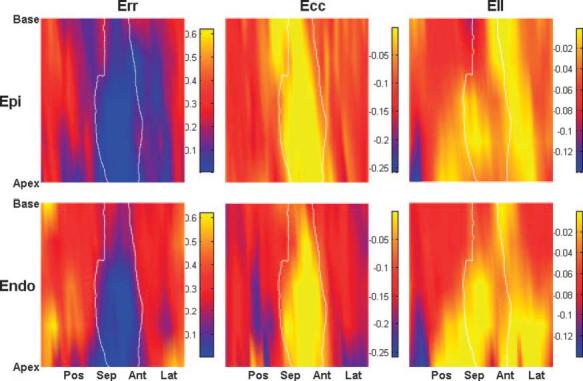
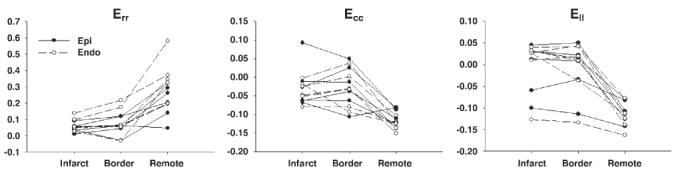
To test the hypothesis that alterations in electrical activation sequence contribute to depressed systolic function in the infarct border zone, we examined the anatomic correlation of abnormal electromechanics and infarct geometry in the canine post-myocardial infarction (MI) heart, using a high-resolution MR-based cardiac electromechanical mapping technique. Three to eight weeks after an MI was created in six dogs, a 247-electrode epicardial sock was placed over the ventricular epicardium under thoracotomy. MI location and geometry were evaluated with delayed hyperenhancement MRI. Three-dimensional systolic strains in epicardial and endocardial layers were measured in five short-axis slices with motion-tracking MRI (displacement encoding with stimulated echoes). Epicardial electrical activation was determined from sock recordings immediately before and after the MR scans. The electrodes and MR images were spatially registered to create a total of 160 nodes per heart that contained mechanical, transmural infarct extent, and electrical data. The average depth of the infarct was 55% (SD 11), and the infarct covered 28% (SD 6) of the left ventricular mass. Significantly delayed activation (>mean + 2SD) was observed within the infarct zone. The strain map showed abnormal mechanics, including abnormal stretch and loss of the transmural gradient of radial, circumferential, and longitudinal strains, in the region extending far beyond the infarct zone. We conclude that the border zone is characterized by abnormal mechanics directly coupled with normal electrical depolarization. This indicates that impaired function in the border zone is not contributed by electrical factors but results from mechanical interaction between ischemic and normal myocardium.
Figures
References
-
- Barr RC, Spach MS. Sampling rates required for digital recording of intracellular and extracellular cardiac potentials. Circulation. 1977;55:40–48. - PubMed
-
- Cohn JN. Post-MI remodeling. Clin Cardiol. 1993;16:II21–II24. - PubMed
-
- Curran-Everett D, Benos D. Guidelines for reporting statistics in journals published by the American Physiological Society. Am J Physiol Heart Circ Physiol. 2004;287:H447–H449. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical