

Surgical stabilisation of the spine compared with a programme of intensive rehabilitation for the management of patients with chronic low back pain: cost utility analysis based on a randomised controlled trial
- PMID: 15911536
- PMCID: PMC558091
- DOI: 10.1136/bmj.38441.429618.8F
Surgical stabilisation of the spine compared with a programme of intensive rehabilitation for the management of patients with chronic low back pain: cost utility analysis based on a randomised controlled trial
Abstract
Objective: To determine whether, from a health provider and patient perspective, surgical stabilisation of the spine is cost effective when compared with an intensive programme of rehabilitation in patients with chronic low back pain.
Design: Economic evaluation alongside a pragmatic randomised controlled trial.
Setting: Secondary care.
Participants: 349 patients randomised to surgery (n = 176) or to an intensive rehabilitation programme (n = 173) from 15 centres across the United Kingdom between June 1996 and February 2002.
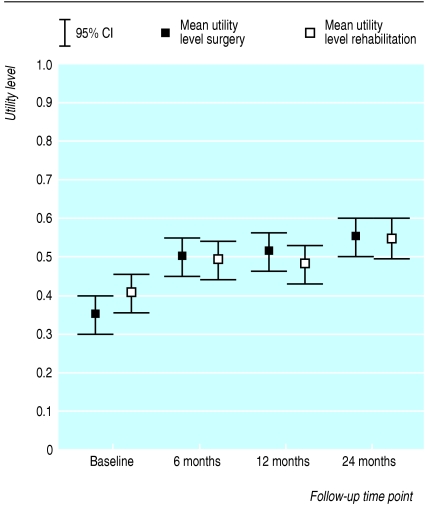
Main outcome measures: Costs related to back pain and incurred by the NHS and patients up to 24 months after randomisation. Return to paid employment and total hours worked. Patient utility as estimated by using the EuroQol EQ-5D questionnaire at several time points and used to calculate quality adjusted life years (QALYs). Cost effectiveness was expressed as an incremental cost per QALY.
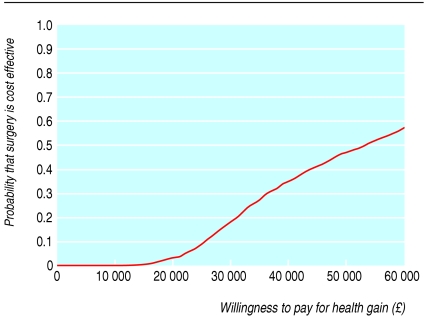
Results: At two years, 38 patients randomised to rehabilitation had received rehabilitation and surgery whereas just seven surgery patients had received both treatments. The mean total cost per patient was estimated to be 7830 pounds sterling (SD 5202 pounds sterling) in the surgery group and 4526 pounds sterling (SD 4155 pounds sterling) in the intensive rehabilitation arm, a significant difference of 3304 pounds sterling (95% confidence interval 2317 pounds sterling to 4291 pounds sterling). Mean QALYs over the trial period were 1.004 (SD 0.405) in the surgery group and 0.936 (SD 0.431) in the intensive rehabilitation group, giving a non-significant difference of 0.068 (-0.020 to 0.156). The incremental cost effectiveness ratio was estimated to be 48,588 pounds sterling per QALY gained (- 279,883 pounds sterling to 372,406 pounds sterling).
Conclusion: Two year follow-up data show that surgical stabilisation of the spine may not be a cost effective use of scarce healthcare resources. However, sensitivity analyses show that this could change-for example, if the proportion of rehabilitation patients requiring subsequent surgery continues to increase.
Figures
References
-
- Maniadakis N, Gray A. The economic burden of back pain in the UK. Pain 2000;84: 95-103. - PubMed
-
- BUPA. Health information, ABC of health, back pain. http://hcd2.bupa.co.uk/fact_sheets/mosby_factsheets/backpain.html (accessed 8 Apr 2005).
-
- Fritzell P, Hägg P, Wessburg P, Nordwall A. 2001 Volvo award winner in clinical studies: lumbar fusion versus nonsurgical treatment for chronic low back pain. A multicenter randomized controlled trial from the Swedish lumbar spine group. Spine 2001;26: 2521-34. - PubMed
-
- Moller H, Hedlund R. Surgery versus conservative management in adult isthmic spondylolisthesis—a prospective randomized study: part 1. Spine 2000;25: 1711-5. - PubMed
-
- Brox JI, Sorensen R, Friis A, Nygaard O, Indahl A, Keller A, et al. Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28: 1913-21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources