

Cardiac dyssynchrony analysis using circumferential versus longitudinal strain: implications for assessing cardiac resynchronization
- PMID: 15911694
- PMCID: PMC2396330
- DOI: 10.1161/CIRCULATIONAHA.104.508457
Cardiac dyssynchrony analysis using circumferential versus longitudinal strain: implications for assessing cardiac resynchronization
Abstract
Background: QRS duration is commonly used to select heart failure patients for cardiac resynchronization therapy (CRT). However, not all patients respond to CRT, and recent data suggest that direct assessments of mechanical dyssynchrony may better predict chronic response. Echo-Doppler methods are being used increasingly, but these principally rely on longitudinal motion (epsilonll). It is unknown whether this analysis yields qualitative and/or quantitative results similar to those based on motion in the predominant muscle-fiber orientation (circumferential; epsiloncc).
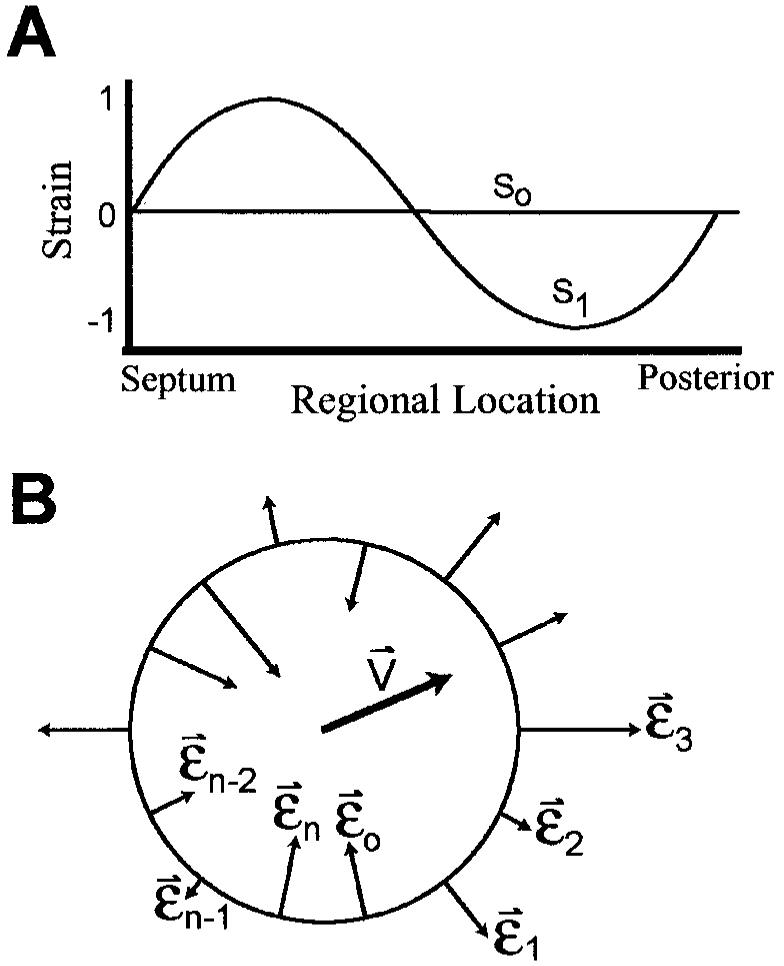
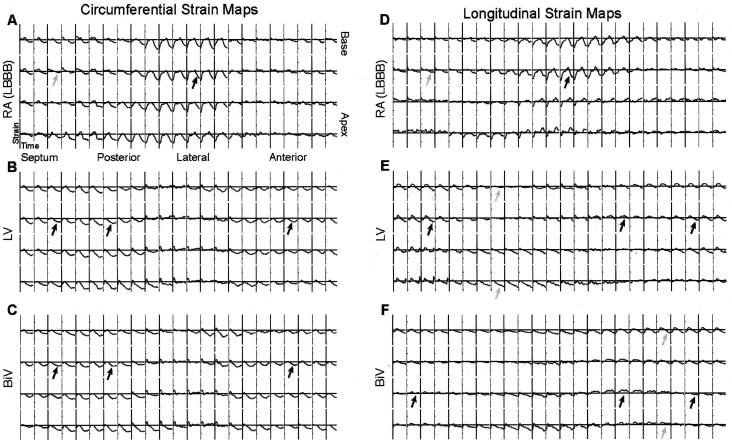
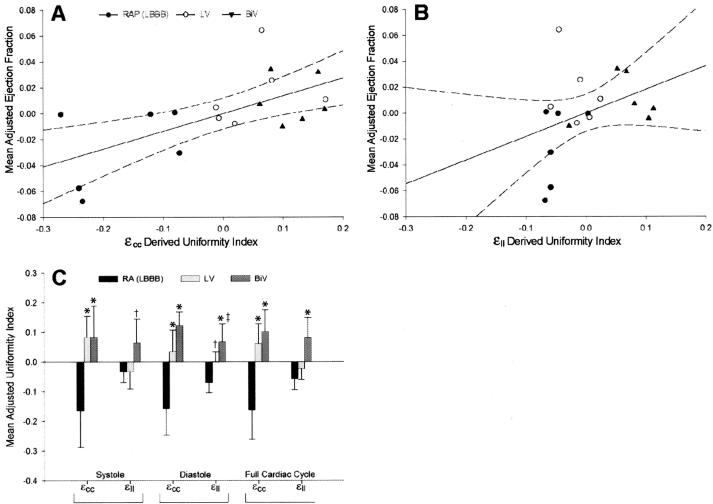
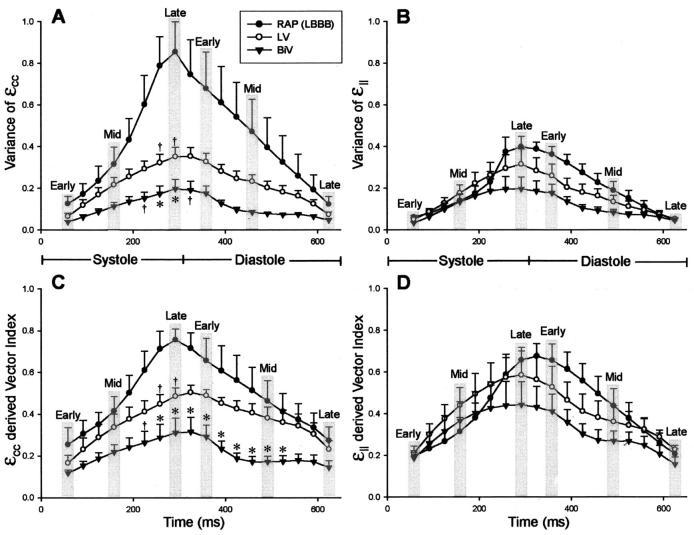
Methods and results: Both epsilonll and epsiloncc strains were calculated throughout the left ventricle from 3D MR-tagged images for the full cardiac cycle in dogs with cardiac failure and a left bundle conduction delay. Dyssynchrony was assessed from both temporal and regional strain variance analysis. CRT implemented by either biventricular (BiV) or left ventricular-only (LV) pacing enhanced systolic function similarly and correlated with improved dyssynchrony based on epsiloncc-based metrics. In contrast, longitudinal-based analyses revealed significant resynchronization with BiV but not LV for the overall cycle and correlated poorly with global functional benefit. Furthermore, unlike circumferential analysis, epsilonll-based indexes indicated resynchronization in diastole but much less in systole and had a lower dynamic range and higher intrasubject variance.
Conclusions: Dyssynchrony assessed by longitudinal motion is less sensitive to dyssynchrony, follows different time courses than those from circumferential motion, and may manifest CRT benefit during specific cardiac phases depending on pacing mode. These results highlight potential limitations to epsilonll-based analyses and support further efforts to develop noninvasive synchrony measures based on circumferential deformation.
Figures
References
-
- Leclercq C, Kass DA. Retiming the failing heart: principles and current clinical status of cardiac resynchronization. J Am Coll Cardiol. 2002;39:194–201. - PubMed
-
- Nelson GS, Berger RD, Fetics BJ, Talbot M, Spinelli JC, Hare JM, Kass DA. Left ventricular or biventricular pacing improves cardiac function at diminished energy cost in patients with dilated cardiomyopathy and left bundle-branch block. Circulation. 2000;102:3053–3059. - PubMed
-
- Yu CM, Chau E, Sanderson JE, Fan K, Tang MO, Fung WH, Lin H, Kong SL, Lam YM, Hill MR, Lau CP. Tissue Doppler echocardiographic evidence of reverse remodeling and improved synchronicity by simultaneously delayed regional contraction after biventricular pacing therapy in heart failure. Circulation. 2002;105:438–445. - PubMed
-
- John Sutton MG, Plappert T, Abraham WT, Smith AL, DeLurgio DB, Leon AR, Loh E, Kocovic DZ, Fisher WG, Ellestad M, Messenger J, Kruger K, Hilpisch KE, Hill MR. Effect of cardiac resynchronization therapy on left ventricular size and function in chronic heart failure. Circulation. 2003;107:1985–1990. - PubMed
-
- McAlister FA, Ezekowitz JA, Wiebe N, Rowe B, Spooner C, Crumley E, Hartling L, Klassen T, Abraham W. Systematic review: cardiac resynchronization in patients with symptomatic heart failure. Ann Intern Med. 2004;141:381–390. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
