

Laparoscopic curative resection of pheochromocytomas
- PMID: 15912041
- PMCID: PMC1357171
- DOI: 10.1097/01.sla.0000164175.26785.06
Laparoscopic curative resection of pheochromocytomas
Abstract
Purpose: Pheochromocytomas are relatively uncommon tumors whose operative resection has clear medical and technical challenges. While the safety and efficacy of laparoscopic adrenalectomy are relatively well documented, few studies with extended follow-up have been conducted to measure the success of the procedure for the most challenging of the adrenal tumors. In addition, several reports question the applicability of a minimally invasive approach for sizeable pheochromocytomas. The purpose of our investigation was to assess the outcomes of laparoscopic adrenalectomy for pheochromocytomas in the largest study to date when performed by experienced laparoscopic surgeons.
Methods: All pheochromocytomas removed by the authors from January 1995 to October 2004 were reviewed under an Institutional Review Board approved protocol. Eighty-five percent were documented in a prospective fashion.
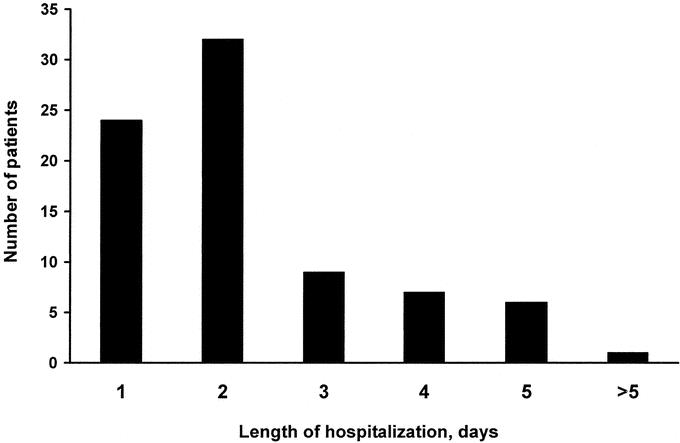
Results: Eighty consecutive patients underwent laparoscopic resection of 81 pheochromocytomas. Seventy-nine were found in the adrenal (42 left, 35 right, 1 bilateral); 2 were extra-adrenal paragangliomas. Eight patients had multiple endocrine neoplasia syndrome. Two lesions were malignant. There were 48 females and 32 males with a mean age of 45 years (range, 15-79 years). Mean tumor size was 5.0 cm (range, 2-12.1 cm); 41 of these lesions were 5 cm in size or larger. Average operative time and blood loss were 169 minutes (range, 69-375 minutes) and 97 mL (range, 20-500 mL), respectively. Intraoperative hypertension (systolic blood pressure, >170 mm Hg) was reported in 53% of patients and hypotension (systolic blood pressure, <90 mm Hg) in 28% of patients. There were no conversions to open surgery. Mean length of stay was 2.3 days (range, 1-10 days). There were 6 perioperative morbidities (7.5%) and no mortalities. No patient required a blood transfusion. No recurrence of endocrinopathy has been documented at a mean follow-up of 21.4 months.
Conclusion: Laparoscopic resection of pheochromocytomas, including large lesions, can be accomplished safely by experienced surgeons. A short hospital stay with minimal operative morbidity and eradication of endocrinopathy support the minimally invasive approach for adrenalectomy in the setting of pheochromocytoma.
Figures
References
-
- Gagner M, Lacroix A, Bolte E. Laparoscopic adrenalectomy in Cushing's syndrome and pheochromocytoma. N Engl J Med. 1992;327:1033. - PubMed
-
- Brunt LM. The positive impact of laparoscopic adrenalectomy on complications of adrenal surgery. Surg Endosc. 2002;16:252–257. - PubMed
-
- Brunt LM, Doherty GM, Norton JA, et al. Laparoscopic adrenalectomy compared to open adrenalectomy for benign adrenal neoplasms. J Am Coll Surg. 1996;183:1–10. - PubMed
-
- Imai T, Kikumori T, Ohiwa M, et al. A case-controlled study of laparoscopic compared with open lateral adrenalectomy. Am J Surg. 1999;178:50–53; discussion 54. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
