

Postoperative outcomes of extremely low birth-weight infants with necrotizing enterocolitis or isolated intestinal perforation: a prospective cohort study by the NICHD Neonatal Research Network
- PMID: 15912048
- PMCID: PMC1359076
- DOI: 10.1097/01.sla.0000164181.67862.7f
Postoperative outcomes of extremely low birth-weight infants with necrotizing enterocolitis or isolated intestinal perforation: a prospective cohort study by the NICHD Neonatal Research Network
Abstract
Objective: Purposes of this study were: 1) to compare mortality and postoperative morbidities (intra-abdominal abscess, wound dehiscence, and intestinal stricture) in extremely low birth weight (ELBW) infants who underwent initial laparotomy or drainage for necrotizing enterocolitis (NEC) or isolated intestinal perforation (IP); 2) to determine the ability to distinguish NEC from IP preoperatively and the importance of this distinction on outcome measures; and 3) to evaluate the association between extent of intestinal disease determined at operation and outcome measures.
Background: ELBW infants who undergo operation for NEC or IP have a postoperative, in-hospital mortality rate of approximately 50%. Whether to perform laparotomy or drainage initially is controversial. Also unknown is the importance of distinguishing NEC from IP and the current ability to make this distinction based on objective data available prior to operation.
Methods: A prospective, multicenter cohort study of 156 ELBW infants at 16 neonatal intensive care units (NICU) within the NICHD Neonatal Research Network.
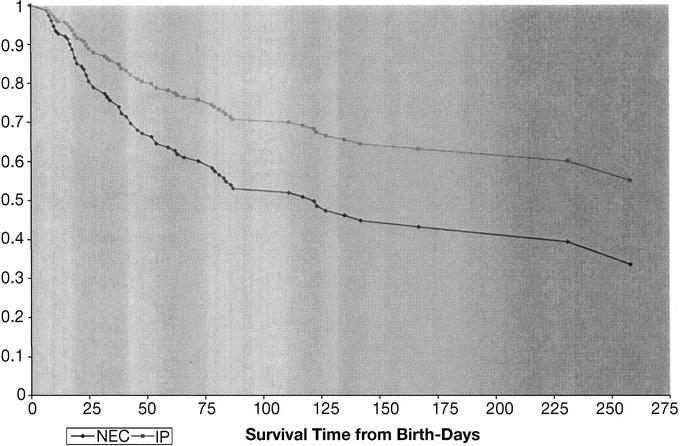
Results: Among the 156 enrolled infants, 80 underwent initial peritoneal drainage and 76 initial laparotomy. Mortality rate was 49% (76 of 156). Ninety-six patients had a preoperative diagnosis of NEC and 60 had presumed IP. There was a high level of agreement between the presumed preoperative diagnosis and intraoperative diagnosis in patients undergoing initial laparotomy (kappa = 0.85). The relative risk for death with a preoperative diagnosis of NEC (versus IP) was 1.4 (95% confidence interval, 0.99-2.1, P = 0.052). The overall incidence of postoperative intestinal stricture was 10.3%, wound dehiscence 4.4%, and intra-abdominal abscess 5.8%, and did not significantly differ between groups undergoing initial laparotomy versus initial drainage.
Conclusions: Survival to hospital discharge after operation for NEC or IP in ELBW neonates remains poor (51%). Patients with a preoperative diagnosis of NEC have a relative risk for death of 1.4 compared with those with a preoperative diagnosis of IP. A distinction can be made preoperatively between NEC and IP based on abdominal radiographic findings and the patient's age at operation. Future randomized trials that compare laparotomy versus drainage would likely benefit from stratification of treatment assignment based on preoperative diagnosis.
Figures
References
-
- Ricketts RR, Jerles ML. Neonatal necrotizing enterocolitis: experience with 100 consecutive surgical patients. World J Surg. 1990;14:600–605. - PubMed
-
- Ketzer de Souza JC, da Motta UIC, Ketzer CR. Prognostic factors of mortality in newborns with necrotizing enterocolitis submitted to exploratory laparotomy. J Pediatr Surg. 2001;36:482–486. - PubMed
-
- Dzakovic A, Notrica DM, O'Brian S, et al. Primary peritoneal drainage for increasing ventilatory requirements in critically ill neonates with necrotizing enterocolitis. J Pediatr Surg. 2001;36:730–732. - PubMed
-
- Cheu HW, Sukarochana K, Lloyd DA. Peritoneal drainage for necrotizing enterocolitis. J Pediatr Surg. 1988;23:557–561. - PubMed
Publication types
MeSH terms
Grants and funding
- U10HD40492/HD/NICHD NIH HHS/United States
- U10 HD027856/HD/NICHD NIH HHS/United States
- U10 HD021373/HD/NICHD NIH HHS/United States
- U10HD40461/HD/NICHD NIH HHS/United States
- K23HD001473/HD/NICHD NIH HHS/United States
- U10 HD021385/HD/NICHD NIH HHS/United States
- U10HD40521/HD/NICHD NIH HHS/United States
- U10HD21373/HD/NICHD NIH HHS/United States
- U10HD27851/HD/NICHD NIH HHS/United States
- U01 HD036790/HD/NICHD NIH HHS/United States
- U10HD40498/HD/NICHD NIH HHS/United States
- U10 HD021364/HD/NICHD NIH HHS/United States
- U10 HD027880/HD/NICHD NIH HHS/United States
- U10 HD040521/HD/NICHD NIH HHS/United States
- U01HD36790/HD/NICHD NIH HHS/United States
- U10HD27856/HD/NICHD NIH HHS/United States
- U10 HD040461/HD/NICHD NIH HHS/United States
- U10 HD040689/HD/NICHD NIH HHS/United States
- U10 HD040492/HD/NICHD NIH HHS/United States
- U10HD27880/HD/NICHD NIH HHS/United States
- U10 HD027853/HD/NICHD NIH HHS/United States
- U10 HD027904/HD/NICHD NIH HHS/United States
- U10 HD021397/HD/NICHD NIH HHS/United States
- U10HD34216/HD/NICHD NIH HHS/United States
- U10HD27871/HD/NICHD NIH HHS/United States
- U10 HD027871/HD/NICHD NIH HHS/United States
- U10 HD027851/HD/NICHD NIH HHS/United States
- K24RR17050/RR/NCRR NIH HHS/United States
- U10HD21364/HD/NICHD NIH HHS/United States
- U10HD27904/HD/NICHD NIH HHS/United States
- U10HD21397/HD/NICHD NIH HHS/United States
- U10HD21385/HD/NICHD NIH HHS/United States
- K24 RR017050/RR/NCRR NIH HHS/United States
- U10 HD034216/HD/NICHD NIH HHS/United States
- U10 HD040498/HD/NICHD NIH HHS/United States
- U10HD27853/HD/NICHD NIH HHS/United States
- K23 HD001473/HD/NICHD NIH HHS/United States
- U10HD40689/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
