

Esophageal perforation in adults: aggressive, conservative treatment lowers morbidity and mortality
- PMID: 15912051
- PMCID: PMC1357179
- DOI: 10.1097/01.sla.0000164183.91898.74
Esophageal perforation in adults: aggressive, conservative treatment lowers morbidity and mortality
Abstract
Objective: To evaluate the outcome of aggressive conservative therapy in patients with esophageal perforation.
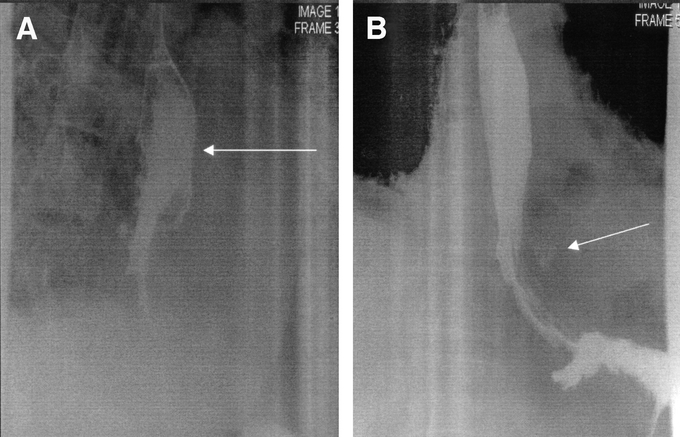
Summary background data: The treatment of esophageal perforation remains controversial with a bias toward early primary repair, resection, and/or proximal diversion. This review evaluates an alternate approach with a bias toward aggressive drainage of fluid collections and frequent CT and gastographin UGI examinations to evaluate progress.
Methods: From 1992 to 2004, 47 patients with esophageal perforation (10 proximal, 37 thoracic) were treated (18 patients early [<24 hours], 29 late). There were 31 male and 16 females (ages 18-90 years). The etiology was iatrogenic (25), spontaneous (14), trauma (3), dissecting thoracic aneurysm (3), and 1 each following a Stretta procedure and Blakemore tube placement.
Results: Six of 10 cervical perforations underwent surgery (3 primary repair, 3 abscess drainage). Nine of 10 perforations healed at discharge. In 37 thoracic perforations, 2 underwent primary repair (1 iatrogenic, 1 spontaneous) and 4 underwent limited thoracotomy. Thirty-4 patients (4 cervical, 28 thoracic) underwent nonoperative treatment. Thirteen of the 14 patients with spontaneous perforation (thoracic) underwent initial nonoperative care. Overall mortality was 4.2% (2 of 47 patients). These deaths represent 2 of 37 thoracic perforations (5.4%). There were no deaths in the 34 patients treated nonoperatively. Esophageal healing occurred in 43 of 45 surviving patients (96%). Subsequent operations included colon interposition in 2, esophagectomy for malignancy in 3, and esophagectomy for benign stricture in 2.
Conclusions: Aggressive treatment of sepsis and control of esophageal leaks leak lowers mortality and morbidity, allow esophageal healing, and avoid major surgery in most patients.
Figures
References
-
- Kiernan PD, Sheridan MJ, Elster E, et al. Thoracic esophageal perforations. South Med J. 2003;96:158–163. - PubMed
-
- Okten I, Cangir AK, Ozdemir N, et al. Management of esophageal perforation. Surg Today. 2001;31:36–39. - PubMed
-
- Gupta NM, Kaman L. Personal management of 57 consecutive patients with esophageal perforation. Am J Surg. 2004;187:58–63. - PubMed
-
- Jougon J, McBride T, Delcambre F, et al. Primary esophageal repair for Boerhaave's syndrome whatever the free interval between perforation and treatment. Eur J Cardiothorac Surg. 2004;25:475–479. - PubMed
-
- Zumbro GL, Anstadt MP, Mawulawde K, et al. Surgical management of esophageal perforation: role of esophageal conservation in delayed perforation. Am Surg. 2002;68:36–40. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
