

Submental Orotracheal Intubation: An Alternative to Tracheotomy in Transfacial Cranial Base Surgery
- PMID: 15912177
- PMCID: PMC1131851
- DOI: 10.1055/s-2004-817694
Submental Orotracheal Intubation: An Alternative to Tracheotomy in Transfacial Cranial Base Surgery
Abstract
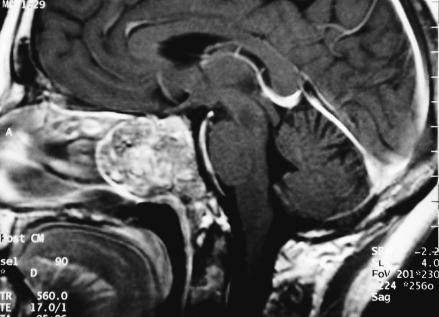
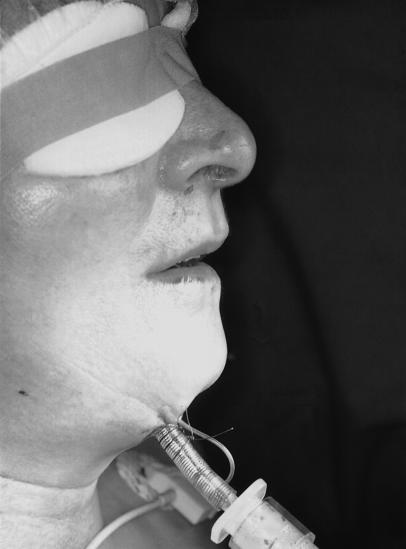
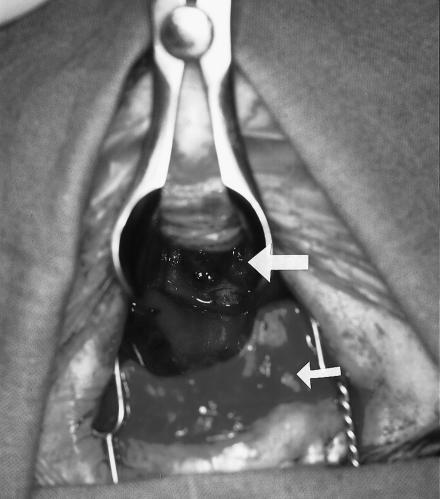
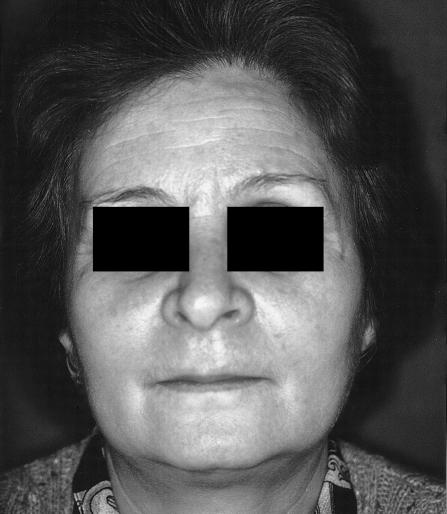
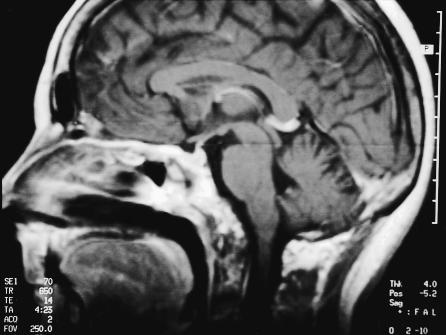
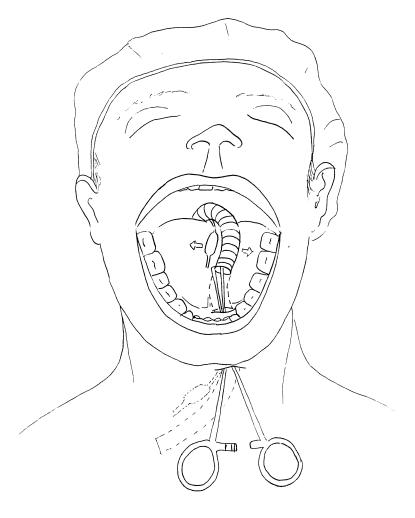
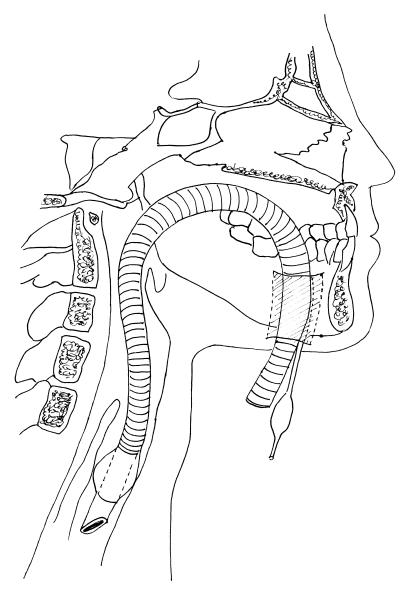
This retrospective study evaluated the safety and efficacy of submental intubation not only for trauma treatment but also for oncological cranial base surgery. The medical records of 24 patients who underwent submental intubation from 1996 to 2002 were reviewed. There were 6 procedures for craniofacial trauma, 12 transmaxillary approaches to the clivus for clivus chordomas, and 6 transmaxillary approaches to the cranial base for chondrosarcomas. Time required for intubation, accidental extubation, postoperative complications, and the healing of intraoral and submental scars were evaluated. The submental orotracheal intubation was completed successfully in all patients. No accidental extubations or tube injuries occurred. The mean time required for intubation was 5 minutes. The only complication was one case of superficial infection of the submental wound. The intraoral and submental accesses healed with minimal scarring in all patients. Submental orotracheal intubation is a useful and safe technique for airway management of craniomaxillofacial traumas and during transfacial approaches to the cranial base. It avoids the complications associated with tracheostomy. It also permits considerable downward retraction of the maxilla after a Le Fort I osteotomy and is associated with good clival exposure. Furthermore, it does not interfere with maxillomandibular fixation at the end of the surgery.
Figures


References
-
- Caron G, Pasquin R, Lessard M, Trepanier C, Landry PE. Submental endotracheal intubation: an alternative to tracheostomy in patients with midfacial and panfacial fractures. J Trauma. 2000;48:235–240. - PubMed
-
- Hall D. Nasotracheal intubation with facial fractures. JAMA. 1989;261:1198.
-
- Schultz RC. Nasotracheal intubation in the presence of facial fractures. Plast Reconstr Surg. 1990;86:1046. - PubMed
-
- Muzzi DM, Losasso TJ, Cucchiara RF. Complications from a nasopharyngeal airway in a patient with a basilar skull fractures. Anesthesiology. 1991;74:366–372. - PubMed
-
- Bahr W, Stoll P. Nasal intubation in the presence of frontobasal fractures. J Oral Maxillofac Surg. 1992;50:445–451. - PubMed
