

Primary Intraosseous Skull Base Cavernous Hemangioma: Case Report
- PMID: 15912181
- PMCID: PMC1131855
- DOI: 10.1055/s-2004-817698
Primary Intraosseous Skull Base Cavernous Hemangioma: Case Report
Abstract
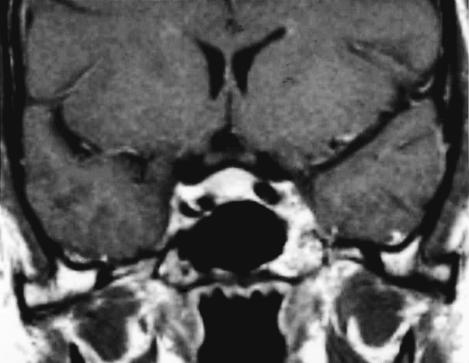
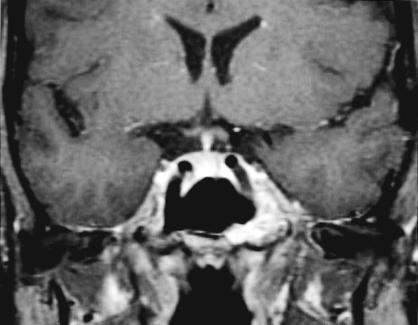
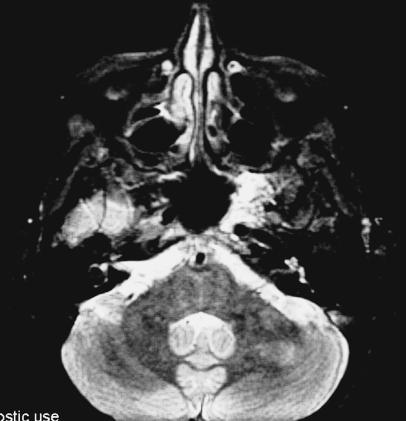
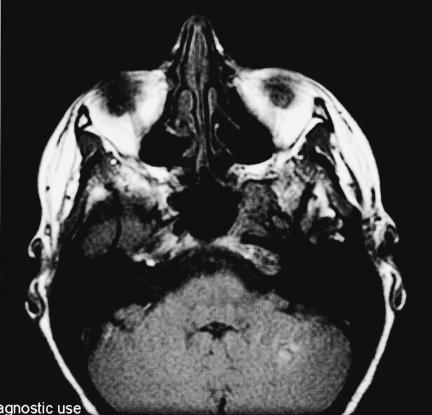
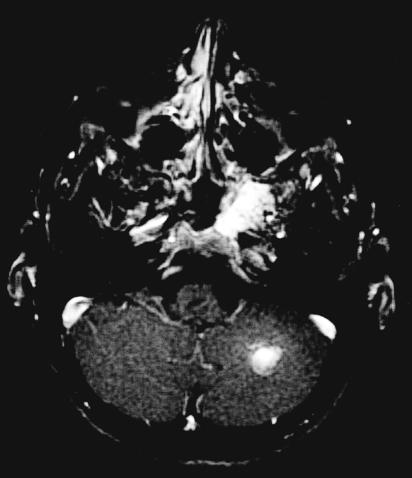
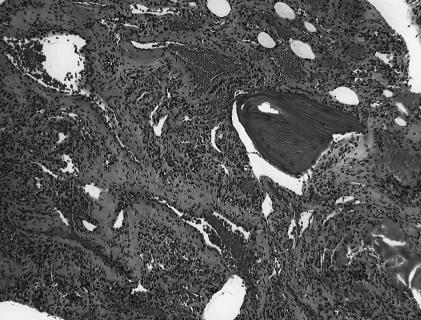
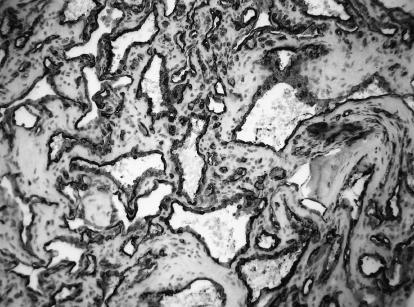
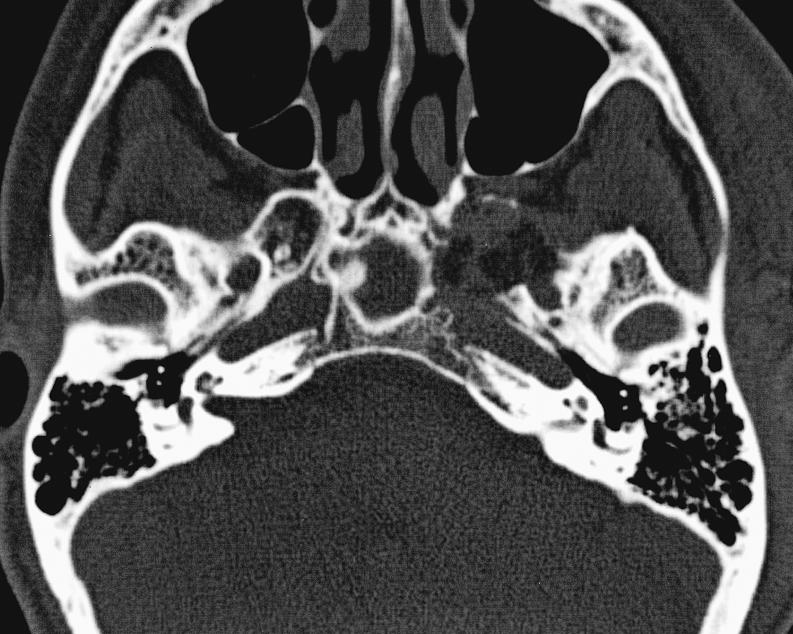
Primary intraosseous cavernous hemangiomas (PICHs) of the skull base are extremely rare tumors. These lesions are most common in the frontal and parietal bones of the calvarium. The authors describe a 40-year-old female who presented with progressive headaches. Serial imaging revealed a contrast-enhancing intraosseous lesion of the lateral body of the sphenoid bone and the greater wing associated with encroachment of the inferior cavernous sinus and mild posterior displacement of the cavernous carotid artery. Follow-up imaging 9 years later revealed slow growth of the lesion. The patient underwent complete excision of the PICH through an extradural frontopolar approach. Pathological examination revealed an intraosseous cavernous hemangioma. PICHs of the skull base can mimic other more common skull base lesions and thus can be difficult to diagnose preoperatively. Diagnosis is usually made at surgery. The authors review the literature regarding the clinical presentation, radiological characteristics, pathological features, and surgical management of PICHs.
Figures







References
-
- Wyke BD. Primary hemangioma of skull. A rare cranial tumour. AJR Am J Roentgenol. 1946;61:302–316. - PubMed
-
- Nakahira M, Kishimoto S, Miura T, Saito H. Intraosseous hemangioma of the vomer: a case report. Am J Rhinol. 1997;11:473–477. - PubMed
-
- Cuesta G, Navarro–Vila C. Intraosseous hemangioma of the zygomatic bone. A case report. Int J Oral Maxillofac Surg. 1992;21:287–291. - PubMed
-
- Ozdemir R, Alagoz S, Uysal AC, Unlu RE, Ortak T, Sensoz O. Intraosseous hemangioma of the mandible: a case report and review of the literature. J Craniofac Surg. 2002;13:38–43. - PubMed
