

High prevalence of glucose-6-phosphate dehydrogenase deficiency without gene mutation suggests a novel genetic mechanism predisposing to ketosis-prone diabetes
- PMID: 15914531
- PMCID: PMC6143174
- DOI: 10.1210/jc.2004-2545
High prevalence of glucose-6-phosphate dehydrogenase deficiency without gene mutation suggests a novel genetic mechanism predisposing to ketosis-prone diabetes
Abstract
Context: Ketosis-prone diabetes (KPD) is mostly observed in males of West African descent and is characterized by phasic or permanent insulin dependence without apparent autoimmune process.
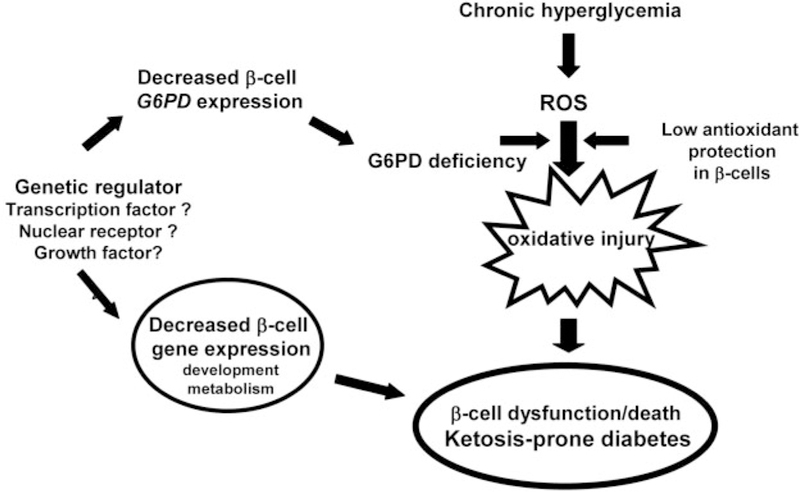
Objective: KPD subjects display a propensity to hyperglycemia-induced acute insulin deficiency, suggesting that they exhibit a propensity to oxidative stress in beta-cells. The enzyme glucose-6-phosphate dehydrogenase (G6PD) is a defense mechanism against oxidative stress, and G6PD deficiency, an X-linked genetic disorder with male predominance, is frequent in West Africans. We hypothesized that mutations in the G6PD gene could predispose to KPD.
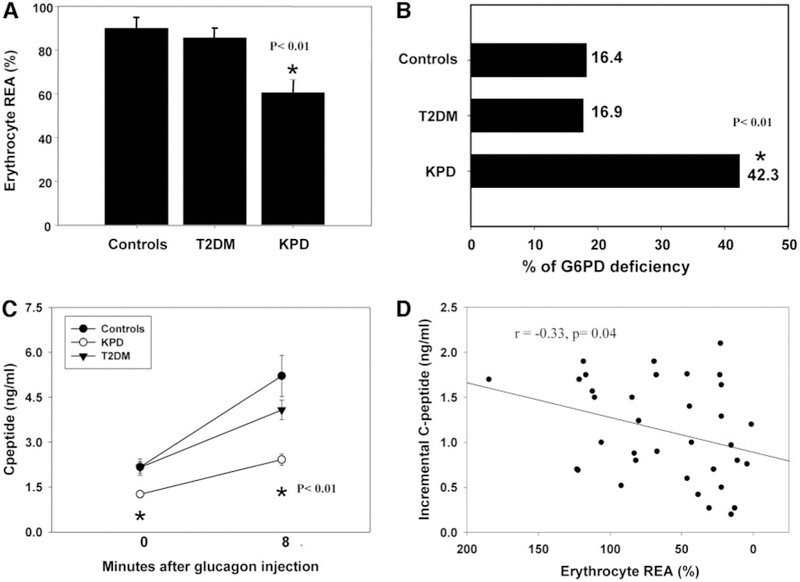
Design: We studied G6PD erythrocyte enzyme activity and the insulin secretory reserve (glucagon-stimulated C peptide) in a cohort of hospitalized West Africans with KPD (n = 59) or type 2 diabetes (T2DM; n = 59) and in normoglycemic controls (n = 55). We also studied the G6PD gene in an extended population of KPD patients (n = 100), T2DM patients (n = 59), and controls (n = 85).
Results: The prevalence of G6PD deficiency was higher in KPD than in T2DM and controls (42.3%; 16.9%; 16.4%; P = 0.01). In KPD, but not in T2DM, insulin deficiency was proportional to the decreased G6PD activity (r = 0.33; P = 0.04). We found no increase in the prevalence of G6PD gene mutations in KPD compared with T2DM and controls. Rather, we found a 20.3% prevalence of G6PD deficiency in KPD without gene mutation.
Conclusions: This study suggests that 1) G6PD deficiency alone is not causative of KPD; and 2) alterations in genes controlling both insulin secretion and G6PD-mediated antioxidant defenses may contribute to the predisposition to KPD in West Africans.
Figures
Similar articles
-
Hyperglycaemia per se does not affect erythrocyte glucose-6-phosphate dehydrogenase activity in ketosis-prone diabetes.Diabetes Metab. 2015 Sep;41(4):326-330. doi: 10.1016/j.diabet.2014.07.002. Epub 2015 Sep 1. Diabetes Metab. 2015. PMID: 26337344
-
PAX4 gene variations predispose to ketosis-prone diabetes.Hum Mol Genet. 2004 Dec 15;13(24):3151-9. doi: 10.1093/hmg/ddh341. Epub 2004 Oct 27. Hum Mol Genet. 2004. PMID: 15509590 Free PMC article.
-
The polymorphism Arg585Gln in the gene of the sterol regulatory element binding protein-1 (SREBP-1) is not a determinant of ketosis prone type 2 diabetes (KPD) in Africans.Diabetes Metab. 2009 Feb;35(1):20-4. doi: 10.1016/j.diabet.2008.06.003. Epub 2008 Dec 4. Diabetes Metab. 2009. PMID: 19062325
-
[Glucose 6-phosphate dehydrogenase deficiency: a protection against malaria and a risk for hemolytic accidents].C R Biol. 2004 Aug;327(8):711-20. doi: 10.1016/j.crvi.2004.07.010. C R Biol. 2004. PMID: 15506519 Review. French.
-
Glucose-6-Phosphate Dehydrogenase Deficiency.Hematol Oncol Clin North Am. 2016 Apr;30(2):373-93. doi: 10.1016/j.hoc.2015.11.006. Hematol Oncol Clin North Am. 2016. PMID: 27040960 Review.
Cited by
-
A mathematical model for ketosis-prone diabetes suggests the existence of multiple pancreatic β-cell inactivation mechanisms.bioRxiv [Preprint]. 2025 Apr 28:2024.06.04.597343. doi: 10.1101/2024.06.04.597343. bioRxiv. 2025. Update in: Elife. 2025 Jul 15;13:RP100193. doi: 10.7554/eLife.100193. PMID: 38895272 Free PMC article. Updated. Preprint.
-
Structure and function of glucose-6-phosphate dehydrogenase-deficient variants in Chinese population.Hum Genet. 2006 Jun;119(5):463-78. doi: 10.1007/s00439-005-0126-5. Epub 2006 Apr 11. Hum Genet. 2006. PMID: 16607506
-
Prevalence and clinical characteristics of lower limb atherosclerotic lesions in newly diagnosed patients with ketosis-onset diabetes: a cross-sectional study.Diabetol Metab Syndr. 2014 Jun 3;6:71. doi: 10.1186/1758-5996-6-71. eCollection 2014. Diabetol Metab Syndr. 2014. PMID: 24926320 Free PMC article.
-
A Rare Case of Ketosis-Prone Type 2 Diabetes With a Unique Human Leukocyte Antigen (HLA) Profile: Genetic and Metabolic Insights.Cureus. 2025 Jan 10;17(1):e77247. doi: 10.7759/cureus.77247. eCollection 2025 Jan. Cureus. 2025. PMID: 39925547 Free PMC article.
-
Syndromes of ketosis-prone diabetes mellitus.Endocr Rev. 2008 May;29(3):292-302. doi: 10.1210/er.2007-0026. Epub 2008 Feb 21. Endocr Rev. 2008. PMID: 18292467 Free PMC article. Review.
References
-
- Mauvais-Jarvis F, Sobngwi E, Porcher R, Riveline JP, Kevorkian JP, Vaisse C, Guillausseau PJ, Charpentier G, Vexiau P, Gautier JF 2004. Ketosis-prone type 2 diabetes in patients of sub-Saharan African origin: clinical pathophysiology and natural history of β-cell dysfunction and insulin resistance. Diabetes 53:645–653 - PubMed
-
- Umpierrez GE, Casals MM, Gebhart SP, Mixon PS, Clark WS, Phillips LS 1995. Diabetic ketoacidosis in obese African-Americans. Diabetes 44:790–795 - PubMed
-
- Poitout V, Robertson RP 2002. Minireview: secondary β-cell failure in type 2 diabetes: a convergence of glucotoxicity and lipotoxicity. Endocrinology 143: 339–342 - PubMed
-
- Prentki M, Joly E, El-Assaad W, Roduit R 2002. Malonyl-CoA signaling, lipid partitioning, and glucolipotoxicity: role in β-cell adaptation and failure in the etiology of diabetes. Diabetes 51(Suppl 3):S405–S413 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
