

Adult tobacco use levels after intensive tobacco control measures: New York City, 2002-2003
- PMID: 15914827
- PMCID: PMC1449302
- DOI: 10.2105/AJPH.2004.058164
Adult tobacco use levels after intensive tobacco control measures: New York City, 2002-2003
Abstract
Objectives: We sought to determine the impact of comprehensive tobacco control measures in New York City.
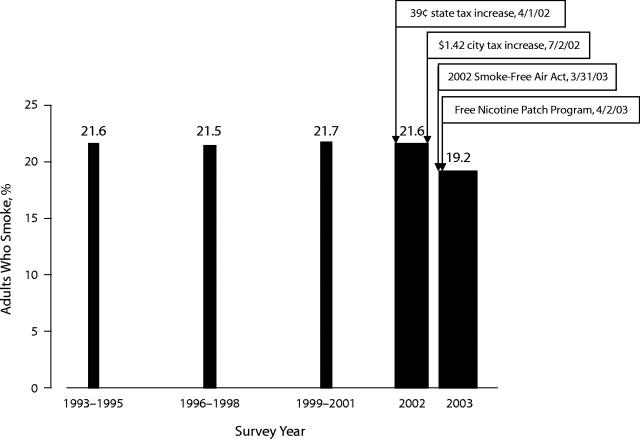
Methods: In 2002, New York City implemented a tobacco control strategy of (1) increased cigarette excise taxes; (2) legal action that made virtually all work-places, including bars and restaurants, smoke free; (3) increased cessation services, including a large-scale free nicotine-patch program; (4) education; and (5) evaluation. The health department also began annual surveys on a broad array of health measures, including smoking.
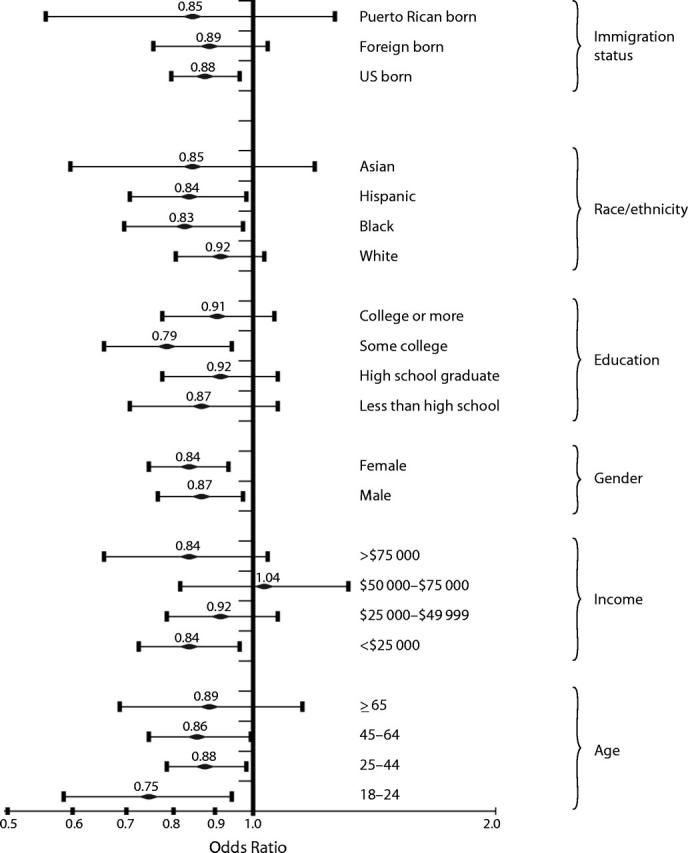
Results: From 2002 to 2003, smoking prevalence among New York City adults decreased by 11% (from 21.6% to 19.2%, approximately 140000 fewer smokers). Smoking declined among all age groups, race/ethnicities, and education levels; in both genders; among both US-born and foreign-born persons; and in all 5 boroughs. Increased taxation appeared to account for the largest proportion of the decrease; however, between 2002 and 2003 the proportion of cigarettes purchased outside New York City doubled, reducing the effective price increase by a third.
Conclusions: Concerted local action can sharply reduce smoking prevalence. However, further progress will require national action, particularly to increase cigarette taxes, reduce cigarette tax evasion, expand education and cessation services, and limit tobacco marketing.
Figures
References
-
- Centers for Disease Control and Prevention. Annual smoking-attributable mortality, years of potential life lost, and economic costs—United States, 1995–1999. MMWR Morb Mortal Wkly Rep.2002;51:300–303. - PubMed
-
- Centers for Disease Control and Prevention. Cigarette smoking-attributable morbidity—United States, 2000. MMWR Morb Mortal Wkly Rep.2003;52:842–844. - PubMed
-
- Centers for Disease Control and Prevention, Office on Smoking and Health. Smoking prevalence among US adults. July 2002. Available at: http://www.cdc.gov/tobacco/research_data/adults_prev/prevali.htm. Accessed January 4, 2005.
-
- New York State Department of Health. Tobacco Use, Cessation, and Exposure to Environmental Tobacco Smoke Among New York State Adults: Behavioral Risk Factor Surveillance System. Albany, NY: New York State Department of Health; 2003. Available at: http://www.health.state.ny.us/nysdoh/tobacco/reports/brfss2001.htm. Accessed January 4, 2005.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
