

doi: 10.1128/AAC.49.6.2546-2549.2005.
Caspofungin in combination with amphotericin B against Candida glabrata
Affiliations
- PMID: 15917570
- PMCID: PMC1140549
- DOI: 10.1128/AAC.49.6.2546-2549.2005
Item in Clipboard
Caspofungin in combination with amphotericin B against Candida glabrata
Antimicrob Agents Chemother.
2005 Jun.
Abstract
The effects of caspofungin combined with amphotericin B were investigated with Candida glabrata. Although in vitro experiments showed an indifferent interaction, the combination regimen was the only therapeutic approach yielding organ sterilization in a murine candidemia model.
Figures
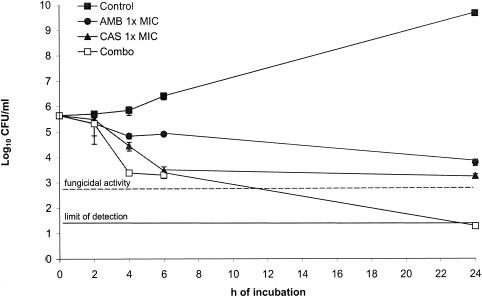
Time-kill studies conducted with C. glabrata 4293. The dashed line represents a >99.9% growth reduction compared with the initial inoculum size. The limit of detection was 20 CFU/ml. Each data point represents the mean ± standard deviation for three independent experiments.
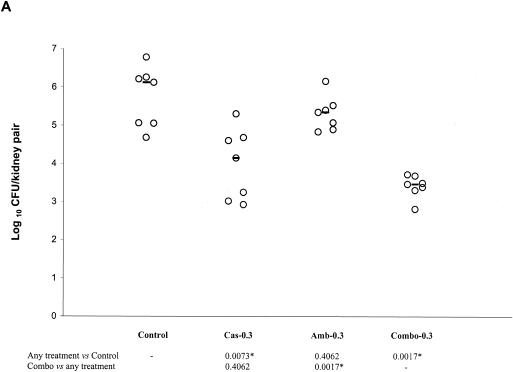
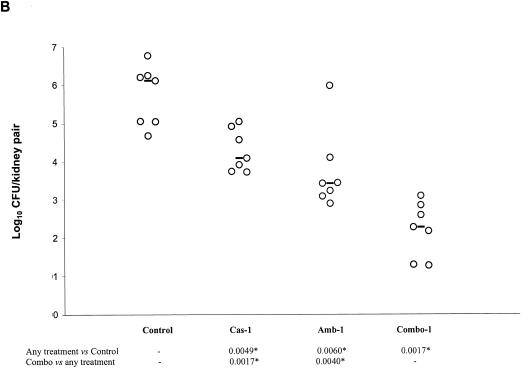
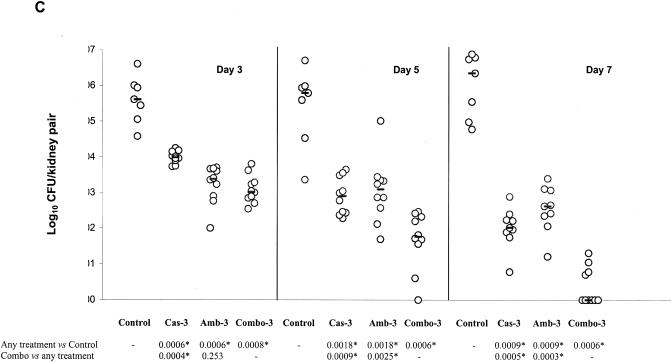
Kidney tissue burden of neutropenic CD1 mice. Study no. 1: panels A and B, the mice were infected intravenously with 2.6 × 108 CFU/mouse of C. glabrata 4293, treated for six consecutive days with CAS at 0.3 or 1 mg/kg/day (Cas-0.3 and Cas-1), with AMB at 0.3 or at 1 mg/kg/day (Amb-0.3 and Amb-1), or with their respective combinations (Combo-0.3 and Combo-1). The mice were sacrificed on day 7 postinfection. Study no. 2: panel C, the mice were infected intravenously with 1.2 × 108 CFU/mouse, treated daily with CAS at 3 mg/kg/day (Cas-3), with AMB at 3 mg/kg/day (Amb-3), or with their combination (Combo-3). Tissue burden experiments were performed on days 3, 5, and 7 postinfection, which corresponded to a total of 2, 4, and 6 days of therapy, respectively. The bars represent the medians. The asterisks at the bottom of panels A, B, and C indicate P values of <0.016.
Kidney tissue burden of neutropenic CD1 mice. Study no. 1: panels A and B, the mice were infected intravenously with 2.6 × 108 CFU/mouse of C. glabrata 4293, treated for six consecutive days with CAS at 0.3 or 1 mg/kg/day (Cas-0.3 and Cas-1), with AMB at 0.3 or at 1 mg/kg/day (Amb-0.3 and Amb-1), or with their respective combinations (Combo-0.3 and Combo-1). The mice were sacrificed on day 7 postinfection. Study no. 2: panel C, the mice were infected intravenously with 1.2 × 108 CFU/mouse, treated daily with CAS at 3 mg/kg/day (Cas-3), with AMB at 3 mg/kg/day (Amb-3), or with their combination (Combo-3). Tissue burden experiments were performed on days 3, 5, and 7 postinfection, which corresponded to a total of 2, 4, and 6 days of therapy, respectively. The bars represent the medians. The asterisks at the bottom of panels A, B, and C indicate P values of <0.016.
Kidney tissue burden of neutropenic CD1 mice. Study no. 1: panels A and B, the mice were infected intravenously with 2.6 × 108 CFU/mouse of C. glabrata 4293, treated for six consecutive days with CAS at 0.3 or 1 mg/kg/day (Cas-0.3 and Cas-1), with AMB at 0.3 or at 1 mg/kg/day (Amb-0.3 and Amb-1), or with their respective combinations (Combo-0.3 and Combo-1). The mice were sacrificed on day 7 postinfection. Study no. 2: panel C, the mice were infected intravenously with 1.2 × 108 CFU/mouse, treated daily with CAS at 3 mg/kg/day (Cas-3), with AMB at 3 mg/kg/day (Amb-3), or with their combination (Combo-3). Tissue burden experiments were performed on days 3, 5, and 7 postinfection, which corresponded to a total of 2, 4, and 6 days of therapy, respectively. The bars represent the medians. The asterisks at the bottom of panels A, B, and C indicate P values of <0.016.
References
-
- Deresinski, S. C., and D. A. Stevens. Caspofungin. 2003. Clin. Infect. Dis. 36:1445-1457. - PubMed
-
- Edmond, M. B., S. E. Wallace, D. K. McClish, M. A. Pfaller, R. N. Jones, and R. P. Wenzel. 1999. Nosocomial bloodstream infections in United States hospitals: a three-year analysis. Clin. Infect. Dis. 29:239-244. - PubMed
-
- Hossain, M. A., G. H. Reyes, L. A. Long, P. K. Mukherjee, and M. A. Ghannoum. 2003. Efficacy of caspofungin combined with amphotericin B against azole-resistant Candida albicans. J. Antimicrob. Chemother. 51:1427-1429. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
