

Construction and clinical significance of a predictive system for prognosis of hepatocellular carcinoma
- PMID: 15918184
- PMCID: PMC4305834
- DOI: 10.3748/wjg.v11.i20.3027
Construction and clinical significance of a predictive system for prognosis of hepatocellular carcinoma
Abstract
Aim: The aims of this study were to explore individualized treatment method for hepatocellular carcinoma (HCC) patients whose maximum tumor size was less than 5 cm to improve prognosis and survival quality.
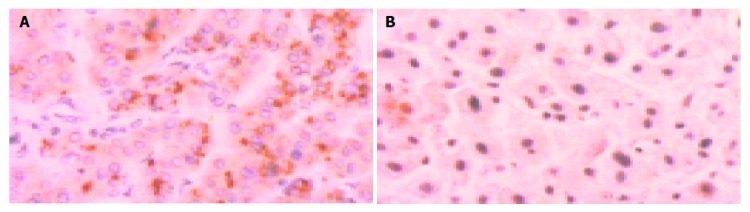
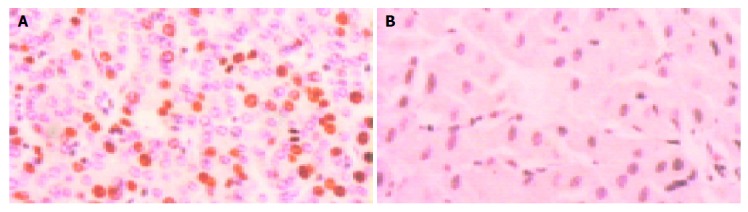
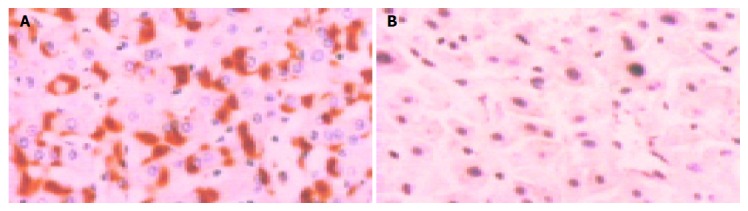
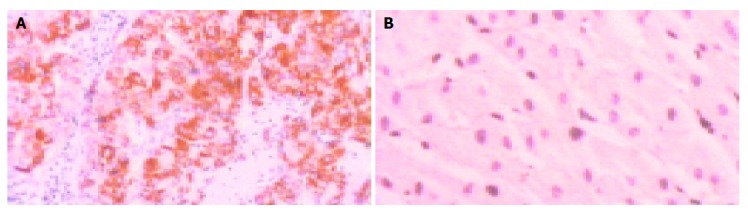
Methods: Thirty cases of primary HCC patients undergoing tumor resection were retrospectively analyzed (resection group). All the tumors were proved as primary HCC with pathologic examination. The patients were divided into two groups according to follow-up results: group A, with tumor recurrence within 1 year after resection; group B, without tumor recurrence within 1 year. Immunohistochemical stainings were performed using 11 kinds of monoclonal antibodies (AFP, c-erbB2, c-met, c-myc, HBsAg, HCV, Ki-67, MMP-2, nm23-H1, P53, and VEGF), and expressing intensities were quantitatively analyzed. Regression equation using factors affecting prognosis of HCC was constructed with binary logistic method. HCC patients undergoing percutaneous microwave coagulation therapy (PMCT) were also retrospectively analyzed (PMCT group). Immunohistochemical stainings of tumor biopsy samples were performed with molecules related to HCC prognosis, staining intensities were quantitatively analyzed, coincidence rate of prediction was calculated.
Results: In resection group, the expressing intensities of c-myc, Ki-67, MMP-2 and VEGF in cancer tissue in group A were significantly higher than those in group B (t = 2.97, P = 0.01; t = 2.42, P = 0.03<0.05; t = 2.57, P = 0.02<0.05; t = 3.43, P = 0.004<0.01, respectively); the expressing intensities of 11 kinds of detected molecules in para-cancer tissue in groups A and B were not significantly different (P>0.05). The regression equation predicting prognosis of HCC is as follows: P(1) = 1/[1+e(-(3.663-0.412mycc-2.187Ki-67c-0.397vegfc))]. It demonstrates that prognosis of HCC in resection group was related with c-myc, Ki-67 and VEGF expressing intensity in cancer tissue. In PMCT group, the expressing intensities of c-myc, Ki-67 and VEGF in cancer tissue in group A were significantly higher than those in group B (t = 4.57, P = 0.000<0.01; t = 2.08, P = 0.04<0.05; t = 2.38, P = 0.02<0.05, respectively); the expressing intensities of c-myc, Ki-67 and VEGF in para-cancer tissue in groups A and B were not significantly different (P>0.05). The coincidence rate of patients undergoing PMCT in group A was 88.00% (22/25), in group B 68.75% (11/16), the total coincidence rate was 80.49% (33/41).
Conclusion: The regression equation is accurate and feasible and could be used for predicting prognosis of HCC, it helps to select treatment method (resection or PMCT) for HCC patients to realize individualized treatment to improve prognosis.
Figures
References
-
- Regimbeau JM, Abdalla EK, Vauthey JN, Lauwers GY, Durand F, Nagorney DM, Ikai I, Yamaoka Y, Belghiti J. Risk factors for early death due to recurrence after liver resection for hepatocellular carcinoma: results of a multicenter study. J Surg Oncol. 2004;85:36–41. - PubMed
-
- Dong BW, Zhang J, Liang P, Yu XL, Su L, Yu DJ, Ji XL, Yu G. Sequential pathological and immunologic analysis of percutaneous microwave coagulation therapy of hepatocellular carcinoma. Int J Hyperthermia. 2003;19:119–133. - PubMed
-
- Levy AE, Kowdley KV. Unresectable hepatocellular carcinoma: the need for an individualized multidisciplinary approach. J Clin Gastroenterol. 2001;33:180–182. - PubMed
-
- Harrison LE, Koneru B, Baramipour P, Fisher A, Barone A, Wilson D, Dela Torre A, Cho KC, Contractor D, Korogodsky M. Locoregional recurrences are frequent after radiofrequency ablation for hepatocellular carcinoma. J Am Coll Surg. 2003;197:759–764. - PubMed
-
- Chen JY, Chau GY, Lui WY, Tsay SH, King KL, Wu CW. Clinicopathologic features and factors related to survival of patients with small hepatocellular carcinoma after hepatic resection. World J Surg. 2003;27:294–298. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
