

Objective perimetry using the multifocal visual evoked potential in central visual pathway lesions
- PMID: 15923511
- PMCID: PMC1772661
- DOI: 10.1136/bjo.2004.053223
Objective perimetry using the multifocal visual evoked potential in central visual pathway lesions
Abstract
Aims: To examine the ability of the multifocal pattern visual evoked potential (mVEP) to detect field loss in neurological lesions affecting the visual pathway from the chiasm to the cortex.
Method: The mVEPs recorded in the clinic were retrospectively reviewed for any cases involving central neurological lesions. Recordings had been performed with the AccuMap V1.3 objective perimeter, which used an array of four bipolar occipital electrodes to provide four differently oriented channels for simultaneous recording. 19 patients with hemianopias were identified. Of these there were 10 homonymous hemianopias with hemifield type loss, two bitemporal hemianopias, and seven homonymous hemianopias with quadrantanopic distribution. A comparison with subjective field results and CT/MRI findings was done to determine the relation between the two methods of visual field mapping and any relation with the anatomical location of the lesion and the mVEP results.
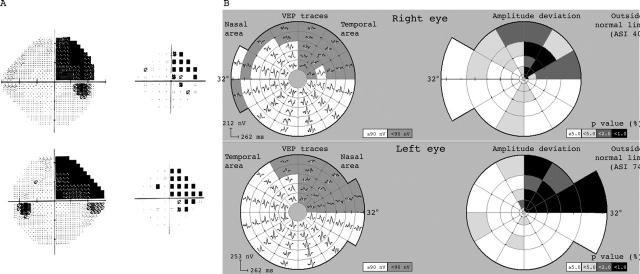
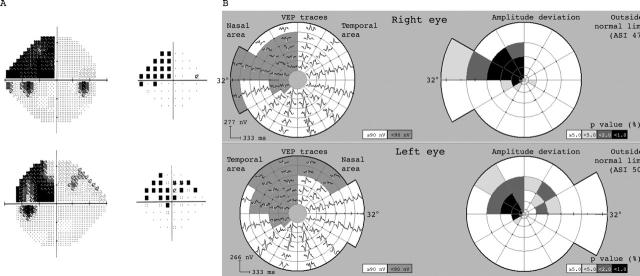
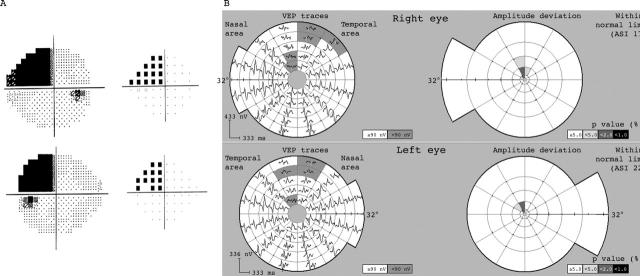
Results: In all hemianopic type cases (12) the defect was demonstrated on the mVEP and showed good correspondence in location of the scotoma (nine homonymous and two bitemporal). The topographic distribution was similar but not identical to subjective testing. Of the seven quadrantanopic type hemianopias, only four were found to have corresponding mVEP losses in the same areas. In the three cases where the mVEP was normal, the type of quadrantanopia had features consistent with an extra-striate lesion being very congruous, complete, and respecting the horizontal meridian.
Conclusions: The mVEP can detect field loss from cortical lesions, but not in some cases of homonymous quadrantanopia, where the lesion may have been in the extra-striate cortex. This supports the concept that the mVEP is generated in V1 striate cortex and that it may be able to distinguish striate from extra-striate lesions. It implies caution should be used when interpreting "functional" loss using the mVEP if the visual field pattern is quadrantic.
Figures


Similar articles
-
Peripheral homonymous hemianopia: correlation between lesion location and visual field defects by means of cytoarchitectonic probabilistic maps.J Neuroophthalmol. 2012 Mar;32(1):5-12. doi: 10.1097/WNO.0b013e31821fc0e9. J Neuroophthalmol. 2012. PMID: 21623227
-
Homonymous quadrantanopia respecting the horizontal meridian. A feature of striate and extrastriate cortical disease.Neurology. 1997 Dec;49(6):1741-6. doi: 10.1212/wnl.49.6.1741. Neurology. 1997. PMID: 9409385
-
Hemifield pattern-reversal visual evoked potentials (VEPs) in retrochiasmal lesions with homonymous visual field defect.Ital J Neurol Sci. 1986 Aug;7(4):437-42. doi: 10.1007/BF02283022. Ital J Neurol Sci. 1986. PMID: 3759417
-
[Hemianopsias in cortical and subcortical lesions of the visual system: what is the difference?].Klin Monbl Augenheilkd. 1988 May;192(5):521-4. doi: 10.1055/s-2008-1050171. Klin Monbl Augenheilkd. 1988. PMID: 3043100 Review. German.
-
[Rehabilitation of lesions in the visual pathways].Klin Monbl Augenheilkd. 2009 Nov;226(11):897-907. doi: 10.1055/s-0028-1109874. Epub 2009 Nov 13. Klin Monbl Augenheilkd. 2009. PMID: 19916150 Review. German.
Cited by
-
Evaluation of hemifield sector analysis protocol in multifocal visual evoked potential objective perimetry for the diagnosis and early detection of glaucomatous field defects.Korean J Ophthalmol. 2014 Feb;28(1):49-65. doi: 10.3341/kjo.2014.28.1.49. Epub 2014 Jan 21. Korean J Ophthalmol. 2014. PMID: 24511212 Free PMC article.
-
Multifocal visual evoked responses to dichoptic stimulation using virtual reality goggles: Multifocal VER to dichoptic stimulation.Doc Ophthalmol. 2006 May;112(3):189-99. doi: 10.1007/s10633-006-0005-y. Epub 2006 Jun 22. Doc Ophthalmol. 2006. PMID: 16794775
-
The importance of the electrophysiological tests in the early diagnosis of ganglion cells and/or optic nerve dysfunction coexisting with pituitary adenoma: an overview.Doc Ophthalmol. 2018 Dec;137(3):193-202. doi: 10.1007/s10633-018-9659-5. Epub 2018 Oct 29. Doc Ophthalmol. 2018. PMID: 30374652 Free PMC article. Review.
-
Multifocal and pattern-reversal visual evoked potentials vs. automated perimetry frequency-doubling technology matrix in optic neuritis.Indian J Ophthalmol. 2013 Feb;61(2):59-64. doi: 10.4103/0301-4738.99638. Indian J Ophthalmol. 2013. PMID: 23412522 Free PMC article.
-
Multifocal Visual Evoked Potential (mfVEP) and Pattern-Reversal Visual Evoked Potential Changes in Patients with Visual Pathway Disorders: A Case Series.Neuroophthalmology. 2015 Aug 25;39(5):220-233. doi: 10.3109/01658107.2015.1074253. eCollection 2015 Oct. Neuroophthalmology. 2015. PMID: 27928359 Free PMC article.
References
-
- Vallar G, Sandroni P, Rusconi ML, et al. Hemianopia, hemianesthesia and spatial neglect: a study with evoked potentials. Neurology 1991;41:1918–22. - PubMed
-
- Biersdorff WR, Bell RA, Beck RW. Pattern visual evoked potentials in patients with homonymous hemianopia. Doc Ophthalmol 1992;80:51–61. - PubMed
-
- Maccolini E, Andreoli A, Valde G, et al. Hemifield pattern-reversal visual evoked potential in retrochiasmal lesions with homonymous visual field defect. Ital J Neurol Sci 1986;7:437–42. - PubMed
-
- Howe JW, Mitchell KW. Visual evoked potentials from quadrantic field stimulation in the investigation of homonymous field defects. In: Barber C, ed. Evoked potentials. Lancaster: MTP Press, 1980:279–83.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical