

Comorbidity and the use of primary care and specialist care in the elderly
- PMID: 15928224
- PMCID: PMC1466877
- DOI: 10.1370/afm.307
Comorbidity and the use of primary care and specialist care in the elderly
Abstract
Purpose: The impact of comorbidity on use of primary care and specialty services is poorly understood. The purpose of this study was to determine the relationship between morbidity burden, comorbid conditions, and use of primary care and specialist services
Methods: The study population was a 5% random sample of Medicare beneficiaries, taken from 1999 Medicare files. We analyzed the number of ambulatory face-to-face patient visits to primary care physicians and specialists for each diagnosis, with each one first considered as the "main" one and then as a comorbid diagnosis to another. Each patient was categorized by extent of total morbidity burden using the Johns Hopkins Adjusted Clinical Group case-mix system.
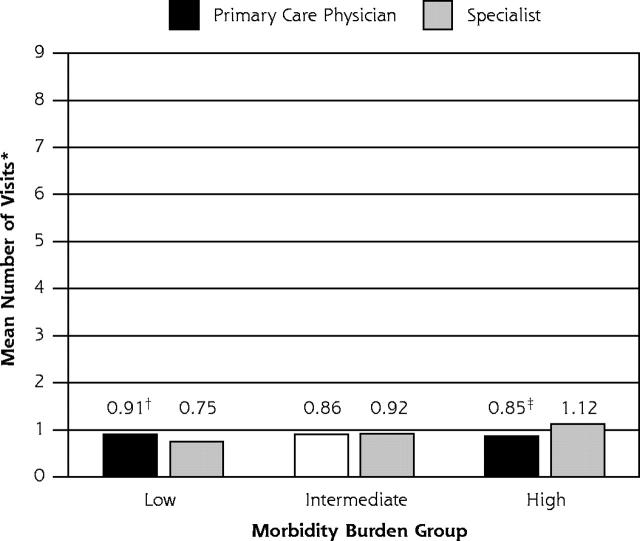
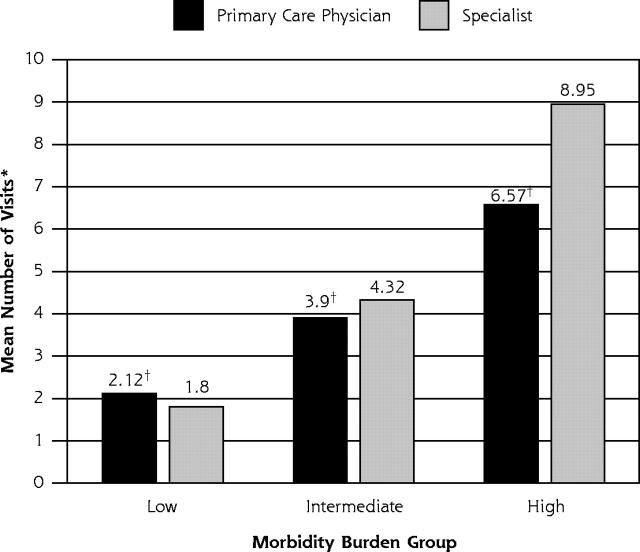
Results: Higher morbidity burden was associated with more visits to specialists, but not to primary care physicians. Patients with most diagnoses had more visits, both to primary care and specialist physicians for comorbid diagnoses than for the main diagnosis itself. Although patients, especially those with high morbidity burdens, generally made more visits to specialists than to primary care physicians, this finding was not always the case. For patients with 66 diagnoses, primary care visits for those diagnoses exceeded specialist visits in all morbidity burden groups; for patients with 87 diagnoses, specialty visits exceeded primary care visits in all morbidity burden groups.
Conclusion: In the elderly, a high morbidity burden leads to higher use of specialist physicians, but not primary care physicians, even for patients with common diagnoses not generally considered to require specialist care. This finding calls for a better understanding of the relative roles of generalists and specialists in the US health services system.
Figures
References
-
- Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med. 2002;162:2269–2276. - PubMed
-
- Starfield B, Forrest CB, Nutting PA, von Schrader S. Variability in physician referral decisions. J Am Board Fam Pract. 2002;15:473–480. - PubMed
-
- Forrest CB, Reid RJ. Passing the baton: HMOs’ influence on referrals to specialty care. Health Aff (Millwood). 1997;16:157–162. - PubMed
-
- Hochberg Y. A sharper Bonferoni procedure for multiple tests of significance. Biometrika. 1988:800–802.
-
- van den Akker M, Buntinx F, Metsemakers JF, Roos S, Knottnerus JA. Multimorbidity in general practice: prevalence, incidence, and determinants of co-occurring chronic and recurrent diseases. J Clin Epidemiol. 1998;51:367–375. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical