

Influence of excess adiposity on exercise fitness and performance in overweight children and adolescents
- PMID: 15930197
- PMCID: PMC1350764
- DOI: 10.1542/peds.2004-1543
Influence of excess adiposity on exercise fitness and performance in overweight children and adolescents
Abstract
Objective: Relatively little is known about how excess body mass affects adolescents' capacity to perform sustained exercise. We hypothesized that most of the difficulty that severely overweight adolescents have with sustained exercise occurs because the metabolic costs of moving excess mass result in use of a high proportion of their total oxygen reserve.
Methods: We compared results from a maximal cycle ergometry fitness test in 129 severely overweight adolescents who had BMIs of 41.5 +/- 9.7 kg/m2 and ages of 14.5 +/- 1.8 years (range: 12.1-17.8 years) and 34 nonoverweight adolescents who had BMIs of 20.1 +/- 2.9 kg/m2 and ages of 14.5 +/- 1.5 years (range: 12.0-18.1 years). Oxygen uptake (Vo2) was compared at 3 times: during a 4-minute period of unloaded cycling (ULVo2), at the lactate threshold estimated by gas exchange (LTVo2), and at maximal exertion (Vo2 max). Heart rate was obtained at rest and at Vo2 max. Participants also completed a 12-minute walk/run performance test to obtain distance traveled (D12) and heart rate.
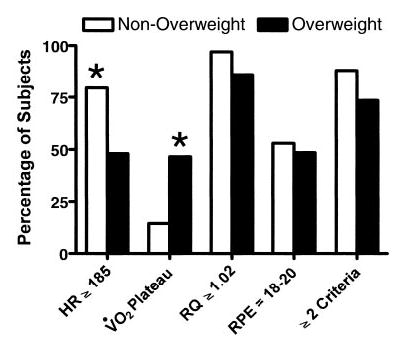
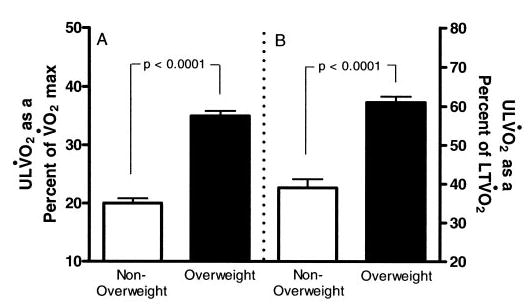
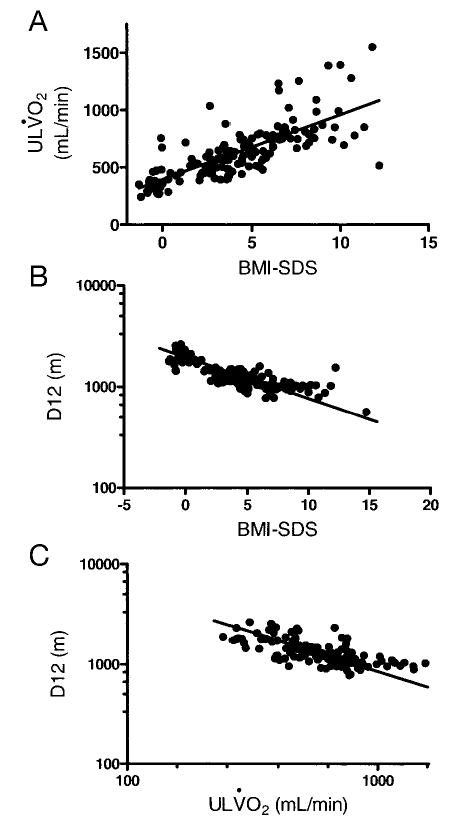
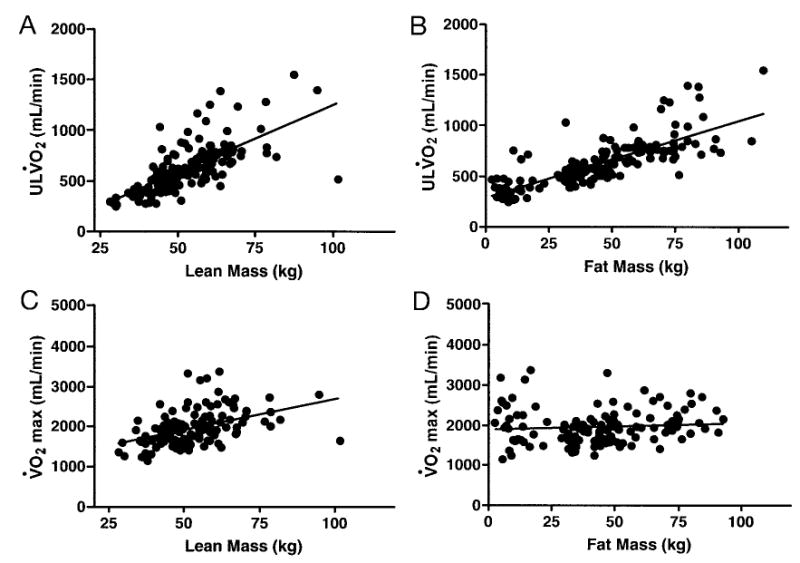
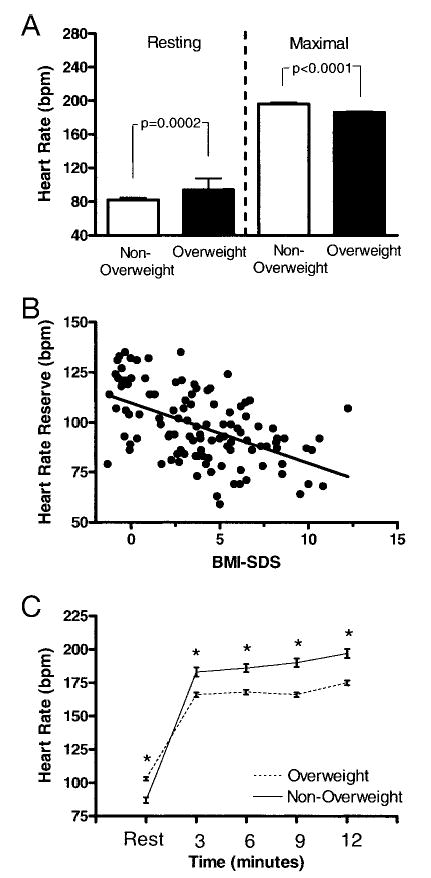
Results: Absolute LTVo2 and Vo2 max and LTVo2 as a percentage of Vo2 max were not different in overweight and nonoverweight adolescents during the cycle test. However, absolute ULVo2 was significantly greater in overweight adolescents: ULVo2 accounted for 35 +/- 8% of Vo2 max (and 63 +/- 15% of LTVo2) in overweight adolescents but only 20 +/- 5% of Vo2 max (and 39 +/- 12% of LTVo2) in nonoverweight adolescents. Resting heart rate before initiating the cycle test was significantly greater in overweight than nonoverweight adolescents (94 +/- 14 vs 82 +/- 15 beats per minute). However, maximal heart rate during the cycle test was significantly lower in overweight adolescents (186 +/- 13 vs 196 +/- 11 beats per minute). During the walk/run test, mean D12 was significantly shorter for overweight than for nonoverweight adolescents (1983 +/- 323 vs 1159 +/- 194 m). D12 was negatively related to BMI SDS (r = -0.81) and to ULVo2 (r = -0.98).
Discussion: Overweight and nonoverweight adolescents had similar absolute Vo2 at the lactate threshold and at maximal exertion, suggesting that overweight adolescents are more limited by the increased cardiorespiratory effort required to move their larger body mass through space than by cardiorespiratory deconditioning. The higher percentage of oxygen consumed during submaximal exercise indicates that overweight adolescents are burdened by the metabolic cost of their excess mass. Their greater oxygen demand during an unloaded task predicted poorer performance during sustained exercise. Exercise prescriptions for overweight adolescents should account for the limited exercise tolerance imposed by excess body mass, focusing on activities that keep demands below lactate threshold so that exercise can be sustained.
Conflict of interest statement
No conflict of interest declared.
Figures
Similar articles
-
Relationships between walk/run performance and cardiorespiratory fitness in adolescents who are overweight.Phys Ther. 2001 Dec;81(12):1889-96. Phys Ther. 2001. PMID: 11736623
-
Ergometric performance and cardiovascular profile of obesity clinic patients.Bull Soc Sci Med Grand Duche Luxemb. 2014;(3):7-24. Bull Soc Sci Med Grand Duche Luxemb. 2014. PMID: 25571669
-
Assessment of Cardiorespiratory Fitness in 8-to-15-Year-Old Children with Overweight/Obesity by Three-Minute Step Test: Association with Degree of Obesity, Blood Pressure, and Insulin Resistance.Indian J Pediatr. 2023 Dec;90(12):1216-1222. doi: 10.1007/s12098-022-04311-z. Epub 2022 Sep 6. Indian J Pediatr. 2023. PMID: 36066791
-
Assessment and interpretation of aerobic fitness in children and adolescents.Exerc Sport Sci Rev. 1994;22:435-76. Exerc Sport Sci Rev. 1994. PMID: 7925551 Review.
-
Energy cost calculations for exercise prescription: an update.Sports Med. 2000 Jul;30(1):17-22. doi: 10.2165/00007256-200030010-00002. Sports Med. 2000. PMID: 10907754 Review.
Cited by
-
Effects of high intensity interval training on sustained reduction in cardiometabolic risk associated with overweight/obesity. A randomized trial.J Exerc Sci Fit. 2022 Apr;20(2):172-181. doi: 10.1016/j.jesf.2022.03.001. Epub 2022 Mar 19. J Exerc Sci Fit. 2022. PMID: 35401768 Free PMC article.
-
Lower Performance in the Six-Minute Walk Test in Obese Youth With Cardiometabolic Risk Clustering.Front Endocrinol (Lausanne). 2018 Nov 27;9:701. doi: 10.3389/fendo.2018.00701. eCollection 2018. Front Endocrinol (Lausanne). 2018. PMID: 30538675 Free PMC article.
-
Nutrient Intake and Physical Exercise Significantly Impact Physical Performance, Body Composition, Blood Lipids, Oxidative Stress, and Inflammation in Male Rats.Nutrients. 2018 Aug 17;10(8):1109. doi: 10.3390/nu10081109. Nutrients. 2018. PMID: 30126091 Free PMC article.
-
Alpha-adrenoceptor-mediated vasoconstriction is not involved in impaired functional vasodilation in the obese Zucker rat.Clin Exp Pharmacol Physiol. 2008 May;35(5-6):611-6. doi: 10.1111/j.1440-1681.2007.04849.x. Epub 2007 Dec 27. Clin Exp Pharmacol Physiol. 2008. PMID: 18177478 Free PMC article.
-
Cardiorespiratory fitness levels and associations with physical activity and body composition in young South African adults from Soweto.BMC Public Health. 2017 Apr 5;17(1):301. doi: 10.1186/s12889-017-4212-0. BMC Public Health. 2017. PMID: 28381219 Free PMC article.
References
-
- Freedman DS, Srinivasan SR, Valdez RA, Williamson DF, Berenson GS. Secular increases in relative weight and adiposity among children over two decades: the Bogalusa Heart Study. Pediatrics. 1997;99:420–426. - PubMed
-
- Ogden CL, Flegal KM, Carroll MD, Johnson CL. Prevalence and trends in overweight among US children and adolescents, 1999–12000. JAMA. 2002;288:1728–1732. - PubMed
-
- Troiano RP, Flegal KM. Overweight children and adolescents: description, epidemiology, and demographics. Pediatrics. 1998;101(3 pt 2):497–504. - PubMed
-
- Must A, Strauss RS. Risks and consequences of childhood and adolescent obesity. Int J Obes Relat Metab Disord. 1999;23(suppl 2):S2–S11. - PubMed
-
- Whitaker RC, Wright JA, Pepe MS, Seidel KD, Dietz WH. Predicting obesity in young adulthood from childhood and parental obesity. N Engl J Med. 1997;337:869–873. - PubMed
