

A clinical return-to-work rule for patients with back pain
- PMID: 15939915
- PMCID: PMC558170
- DOI: 10.1503/cmaj.1041159
A clinical return-to-work rule for patients with back pain
Abstract
Background: Tools for early identification of workers with back pain who are at high risk of adverse occupational outcome would help concentrate clinical attention on the patients who need it most, while helping reduce unnecessary interventions (and costs) among the others. This study was conducted to develop and validate clinical rules to predict the 2-year work disability status of people consulting for nonspecific back pain in primary care settings.
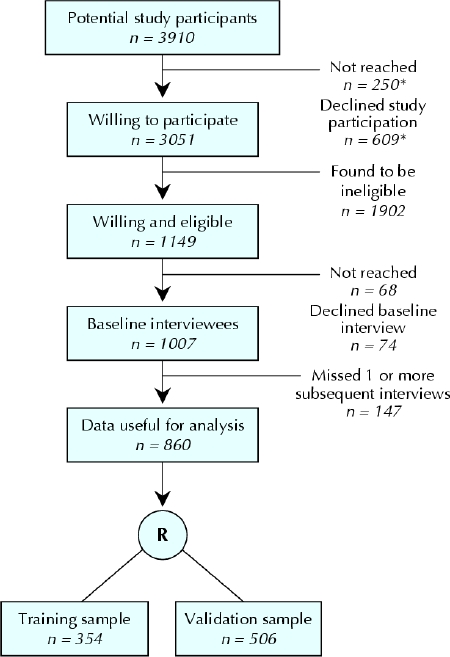
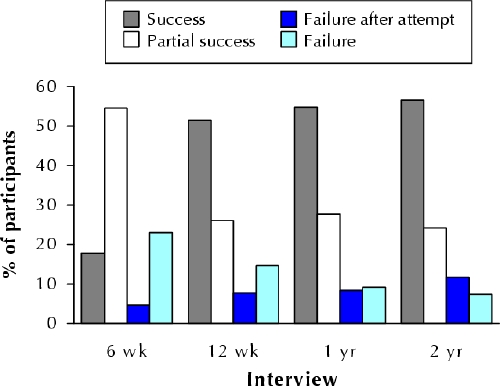
Methods: This was a 2-year prospective cohort study conducted in 7 primary care settings in the Quebec City area. The study enrolled 1007 workers (participation, 68.4% of potential participants expected to be eligible) aged 18-64 years who consulted for nonspecific back pain associated with at least 1 day's absence from work. The majority (86%) completed 5 telephone interviews documenting a large array of variables. Clinical information was abstracted from the medical files. The outcome measure was "return to work in good health" at 2 years, a variable that combined patients' occupational status, functional limitations and recurrences of work absence. Predictive models of 2-year outcome were developed with a recursive partitioning approach on a 40% random sample of our study subjects, then validated on the rest.
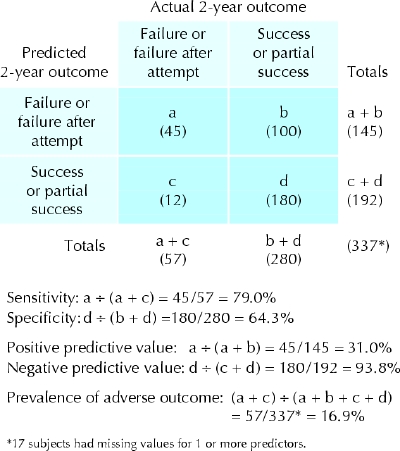
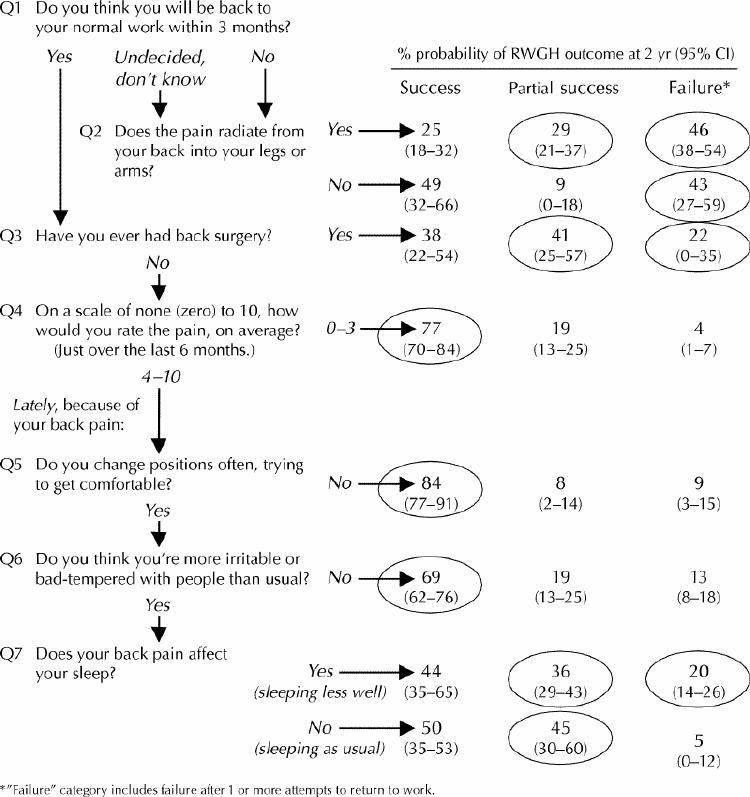
Results: The best predictive model included 7 baseline variables (patient's recovery expectations, radiating pain, previous back surgery, pain intensity, frequent change of position because of back pain, irritability and bad temper, and difficulty sleeping) and was particularly efficient at identifying patients with no adverse occupational outcome (negative predictive value 78%- 94%).
Interpretation: A clinical prediction rule accurately identified a large proportion of workers with back pain consulting in a primary care setting who were at a low risk of an adverse occupational outcome.
Figures
Comment in
-
Clinical prediction rule for return to work after back pain.CMAJ. 2005 Jun 7;172(12):1575-6. doi: 10.1503/cmaj.050530. CMAJ. 2005. PMID: 15939917 Free PMC article. No abstract available.
-
An algorithm comprising 7 baseline variables predicted the 2-year work disability status in nonspecific back pain.ACP J Club. 2005 Nov-Dec;143(3):81. ACP J Club. 2005. PMID: 16262238 No abstract available.
References
-
- Hart LG, Deyo RA, Cherkin DC. Physician office visits for low back pain: frequency, clinical evaluation, and treatment patterns from a US national survey. Spine 1995;20:11-9. - PubMed
-
- Rapoport J, Jacobs P, Bell NR, Klarenbach S. Refining the measurement of the economic burden of chronic diseases in Canada. Chronic Dis Can Winter 2004;25(1):13-21. - PubMed
-
- Druss B. The most expensive medical conditions in America. Health Affairs 2002;21(4):105-11. - PubMed
-
- Bigos S, Bowyer O, Braen G, et al. Acute low back problems in adults. [Clinical Practice Guideline no 14.] Rockville (MD): Agency for Health Care Policy and Research, Public Health Service, US Department of Health and Human Services; 1994. Publication no 95-0642.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials