

Interfractional anatomic variation in patients treated with respiration-gated radiotherapy
- PMID: 15940209
- PMCID: PMC5723469
- DOI: 10.1120/jacmp.v6i2.2048
Interfractional anatomic variation in patients treated with respiration-gated radiotherapy
Abstract
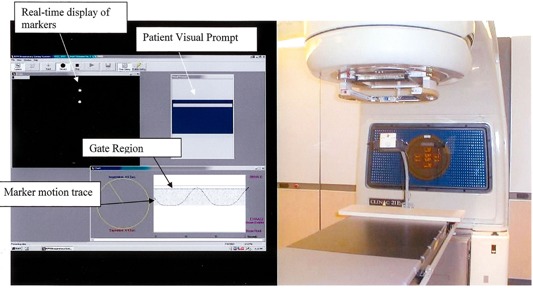
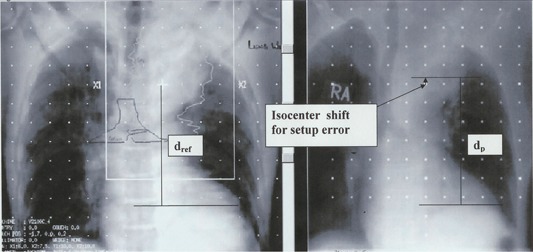
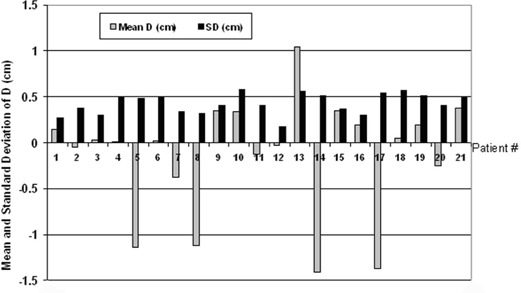
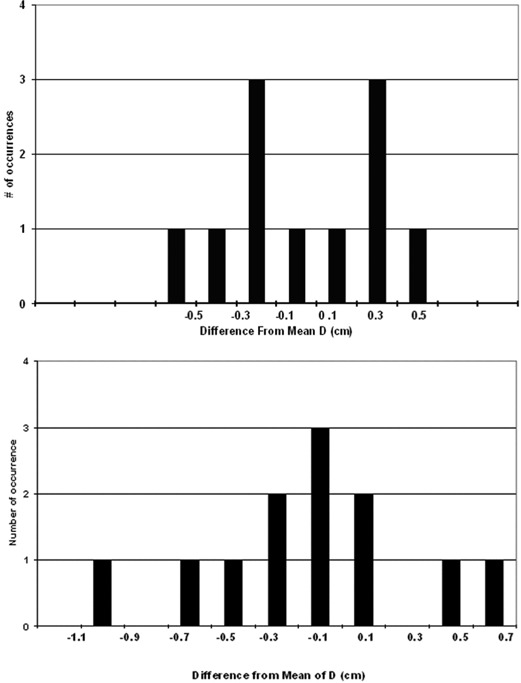
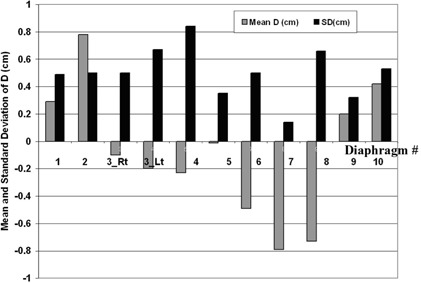
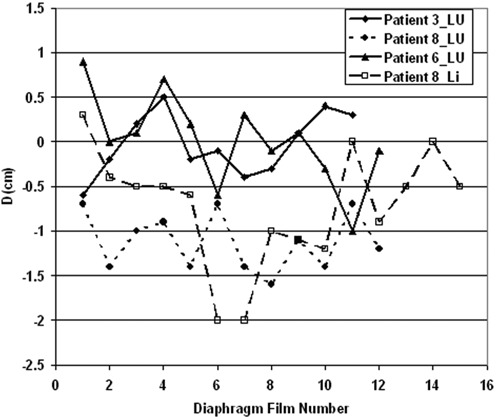
As quality assurance for respiration-gated treatments using the Varian RPM system, we monitor interfractional diaphragm variation throughout treatment using extra anterior-posterior (AP) portal images. We measure the superior-inferior (SI distance between one or more bony landmarks and the ipsilateral diaphragm dome in each such radiograph and calculate its difference, D, from the corresponding distance in a planning CT scan digitally reconstructed radiograph (DRR). For each patient, the mean of D represents the systematic diaphragm displacement, and the standard deviation of D represents random diaphragm variations and is a measure of interfractional gating reproducibility. We present results for 31 sequential patients (21 lung, 10 liver tumors), each with at least 8 such portal images. For all patients, the gate included end-exhale. The patient-specific duty cycle ranged from 30% to 60%. All patients received customized audio prompting for simulation and treatment, and 14 patients also received visual prompting. Respiration-synchronized fluoroscopic movies taken at a conventional simulator revealed patient-specific diaphragm excursions from 1.0 cm to 5.0 cm and diaphragm excursion within the gate from 0.5 cm to 1.0 cm, demonstrating a significant reduction of intra-fractional diaphragm (and by inference tumor) motion by respiratory gating. One standard deviation of the systematic displacement (the mean of D) was 0.63 cm and 0.48 cm for the lung and liver patient groups, respectively. The average +/-1 SD of the random displacements (i.e., the average of the standard deviations of D) was 0.42 +/- 0.11 cm and 0.50 +/- 0.19 for the two groups, respectively. The similar magnitude of the systematic and random displacements suggests that both derive from a common distribution of interfractional variations. Combining visual with audio prompting did not significantly improve performance, as judged by D. Guided by these portal images, field changes were made during the course of treatment for 6 patients (1 lung, 5 liver).
Figures
Similar articles
-
Evaluation of respiratory movement during gated radiotherapy using film and electronic portal imaging.Int J Radiat Oncol Biol Phys. 2002 Feb 1;52(2):522-31. doi: 10.1016/s0360-3016(01)02681-5. Int J Radiat Oncol Biol Phys. 2002. PMID: 11872300
-
Respiration-correlated spiral CT: a method of measuring respiratory-induced anatomic motion for radiation treatment planning.Med Phys. 2003 Jan;30(1):88-97. doi: 10.1118/1.1531177. Med Phys. 2003. PMID: 12557983
-
Quantifying the predictability of diaphragm motion during respiration with a noninvasive external marker.Med Phys. 2003 Apr;30(4):505-13. doi: 10.1118/1.1558675. Med Phys. 2003. PMID: 12722802 Clinical Trial.
-
Respiratory gating for liver tumors: use in dose escalation.Int J Radiat Oncol Biol Phys. 2003 Mar 1;55(3):659-68. doi: 10.1016/s0360-3016(02)03941-x. Int J Radiat Oncol Biol Phys. 2003. PMID: 12573753
-
Computed tomography guided management of interfractional patient variation.Semin Radiat Oncol. 2005 Jul;15(3):168-79. doi: 10.1016/j.semradonc.2005.01.007. Semin Radiat Oncol. 2005. PMID: 15983942 Review.
Cited by
-
Advancing the Collaboration Between Imaging and Radiation Oncology.Semin Radiat Oncol. 2024 Oct;34(4):402-417. doi: 10.1016/j.semradonc.2024.07.005. Semin Radiat Oncol. 2024. PMID: 39271275 Review.
-
Endobronchially Implanted Real-Time Electromagnetic Transponder Beacon-Guided, Respiratory-Gated SABR for Moving Lung Tumors: A Prospective Phase 1/2 Cohort Study.Adv Radiat Oncol. 2023 Apr 18;8(5):101243. doi: 10.1016/j.adro.2023.101243. eCollection 2023 Sep-Oct. Adv Radiat Oncol. 2023. PMID: 37408673 Free PMC article.
-
Perturbation of water-equivalent thickness as a surrogate for respiratory motion in proton therapy.J Appl Clin Med Phys. 2016 Mar 8;17(2):368-378. doi: 10.1120/jacmp.v17i2.5795. J Appl Clin Med Phys. 2016. PMID: 27074459 Free PMC article.
-
Dynamic gating window for compensation of baseline shift in respiratory-gated radiation therapy.Med Phys. 2011 Apr;38(4):1912-8. doi: 10.1118/1.3556588. Med Phys. 2011. PMID: 21626924 Free PMC article.
-
Tumor trailing strategy for intensity-modulated radiation therapy of moving targets.Med Phys. 2008 May;35(5):1718-33. doi: 10.1118/1.2900108. Med Phys. 2008. PMID: 18561647 Free PMC article.
References
-
- Langen KM, Jones DTL. Organ motion and its management. Int J Radiat Oncol Biol Phys. 2001;50:265–278. - PubMed
-
- Mechalakos J, Yorke E, Mageras G, et al. Dosimetric effect of respiratory motion in external beam radiotherapy of the lung. Radiother Oncol. 2004;71:191–200. - PubMed
-
- Tada T, Minakuchi K, Fujioka T, et al. Lung cancer: Intermittent irradiation synchronized with respiratory motion—Results of a pilot study. Radiology. 1998;207:779–783. - PubMed
-
- Shirato H, Shimizu S, Kunieda T, et al. Physical aspects of a real‐time tumor‐tracking system for gated radiotherapy. Int J Radiat Oncol Biol Phys. 2000;48:1187–1195. - PubMed
-
- Kubo HD, Hill BC. Respiration gated radiotherapy treatment: A technical study. Phys Med Biol. 1996;41:83–91. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
