

Review
Epub 2005 Jun 3.
Inhibition and regression of atherosclerotic lesions
Affiliations
- PMID: 15940346
- PMCID: PMC1360606
Item in Clipboard
Review
Inhibition and regression of atherosclerotic lesions
Acta Biochim Pol.
2005.
Abstract
Atherosclerosis, once believed to be a result of a slow, irreversible process resulting from lipid accumulation in arterial walls, is now recognized as a dynamic process with reversibility. Liver-directed gene therapy for dyslipidemia aims to treat patients who are not responsive to currently available primary and secondary prevention. Moreover, gene therapy strategies have also proved valuable in studying the dynamics of atherosclerotic lesion formation, progression, and remodeling in experimental animals. Recent results on the long-term effect of gene therapy suggest that hepatic expression of therapeutic genes suppresses inflammation and has profound effects on the nature of the atherogenic process.
Figures
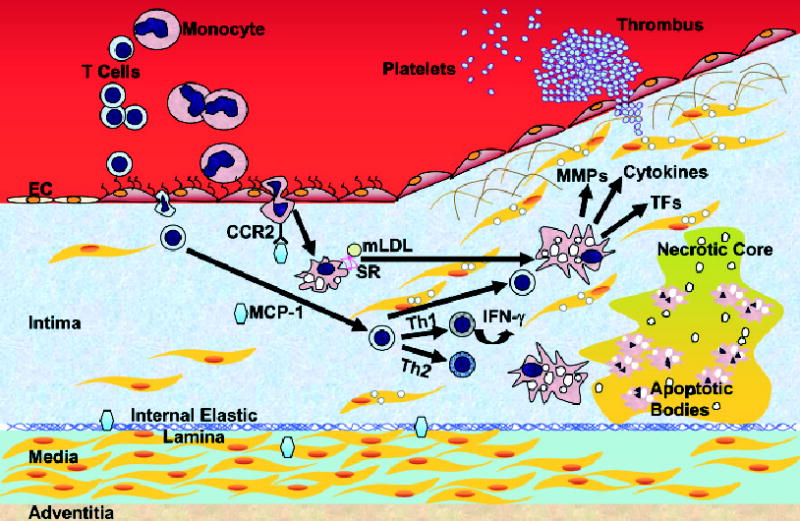
Monocytes and T-leukocytes do not adhere to ECs under normal conditions. 1. Adhesion. When ECs undergo inflammatory activation they express adhesion molecules, and leukocytes are trapped by ECs. 2. Transmigration. Once adherent, leukocytes migrate into the intima. 3. Foam cell formation. In the intima, monocytes differentiate into macrophages and take up lipids. 4. Progression. T cells are activated and further stimulate macrophages. SMCs of the media migrate to the top of the intima to form a fibrous cap over the lipid core. Further activation of macrophages produces MMPs that degrade the extracellular matrix and weaken the fibrous cap. 5. Plaque rupture. When the plaque ruptures, it allows the blood to contact to the procoagulant protein, tissue factor, and activate the coagulant cascade. Macrophages eventually die in a central core by apoptosis or necrosis, which forms a necrotic core in the lesion. IFN-γ, interferon-γ; MCP-1, monocyte chemoattractant protein-1; mLDL, modified LDL; MMP, matrix metalloproteinase; SR, scavenger receptors; TF, tissue factor. Note: Mast cells play an important role in atherogenesis. The interaction of the chemokine receptor CCR3 on the surface of mast cells and eotaxin, a chemoattractant, may facilitate the trans-migration of these cells. In the intima, they undergo degranulation and release factors that contribute to atherogenesis. Mast cells are not indicated.
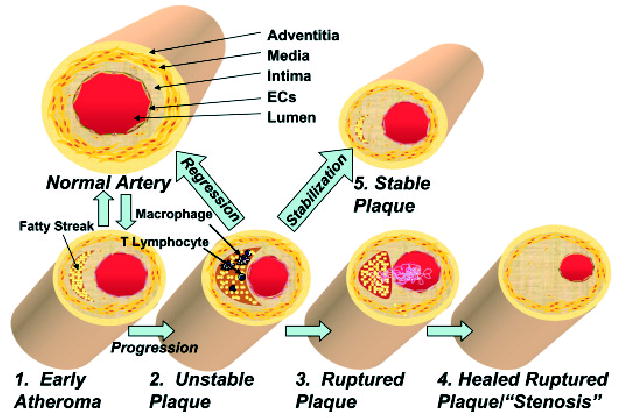
The normal human coronary artery has a trilaminar structure. 1. Early atherosclerotic lesions. In early atherogenesis, migration of immune cells and the accumulation of lipids in macrophages lead to the formation of fatty streaks. These early lesions frequently regress spontaneously. 2. Vulnerable plaque. If inflammatory conditions persist, the lipid core grows. Further activation of macrophages secretes matrix degrading enzymes and weakens the fibrous cap, which leads to vulnerable plaques prone to rupture. 3. Plaque rupture. Disruption of the fibrous cap causes the direct contact of blood components to tissue factor and initiates coagulation. This leads to the formation of the thrombus. 4. Stenosis. A wound healing response stimulates smooth muscle cell migration and collagen synthesis. This process results in a thick fibrous cap and expansion of the intima, which constricts the lumen. 5. Stabilization. Drug treatment or gene therapy for dyslipidemia remodels the nature of the vulnerable plaques, which reduces the incidence of acute coronary events. 6. Regression. Advanced atherosclerotic lesions could be regressed under aggressive lipid lowering or drug treatments.
Similar articles
-
Recent advances in liver-directed gene therapy for dyslipidemia.Curr Atheroscler Rep. 2002 May;4(3):199-207. doi: 10.1007/s11883-002-0020-8. Curr Atheroscler Rep. 2002. PMID: 11931717 Review.
-
Improved animal models for testing gene therapy for atherosclerosis.Hum Gene Ther Methods. 2014 Apr;25(2):106-14. doi: 10.1089/hgtb.2013.199. Epub 2014 Feb 14. Hum Gene Ther Methods. 2014. PMID: 24528162 Free PMC article.
-
Therapeutic gene targeting approaches for the treatment of dyslipidemias and atherosclerosis.Curr Opin Lipidol. 2013 Apr;24(2):116-22. doi: 10.1097/MOL.0b013e32835da13c. Curr Opin Lipidol. 2013. PMID: 23314926 Review.
-
Liver-directed gene transfer vectors.Hum Gene Ther. 1998 Sep 20;9(14):1975-81. doi: 10.1089/hum.1998.9.14-1975. Hum Gene Ther. 1998. PMID: 9759925 Review.
-
Prospect and progress of gene therapy in treating atherosclerosis.Expert Opin Biol Ther. 2015;15(12):1699-712. doi: 10.1517/14712598.2015.1084282. Epub 2015 Aug 31. Expert Opin Biol Ther. 2015. PMID: 26328616 Review.
Cited by
-
If It's Not One Thing, It's Another: An Inverse Relationship of Malignancy and Atherosclerotic Disease.PLoS One. 2015 May 22;10(5):e0126855. doi: 10.1371/journal.pone.0126855. eCollection 2015. PLoS One. 2015. PMID: 26000958 Free PMC article.
-
Lipid lowering by hydroalcoholic extracts of Amaranthus caudatus L. induces regression of rabbits atherosclerotic lesions.Lipids Health Dis. 2011 May 28;10:89. doi: 10.1186/1476-511X-10-89. Lipids Health Dis. 2011. PMID: 21619685 Free PMC article.
-
Alteration of actin dependent signaling pathways associated with membrane microdomains in hyperlipidemia.Proteome Sci. 2015 Dec 1;13:30. doi: 10.1186/s12953-015-0087-0. eCollection 2015. Proteome Sci. 2015. PMID: 26628893 Free PMC article.
References
-
- Aikawa M, Rabkin E, Okada Y, Voglic SJ, Clinton SK, Brinckerhoff CE, Sukhova GK, Libby P. Lipid lowering by diet reduces matrix metalloproteinase activity and increases collagen content of rabbit atheroma: a potential mechanism of lesion stabilization. Circulation. 1998a;97:2433–2444. - PubMed
-
- Aikawa M, Rabkin E, Voglic SJ, Shing H, Nagai R, Schoen FJ, Libby P. Lipid lowering promotes accumulation of mature smooth muscle cells expressing smooth muscle myosin heavy chain isoforms in rabbit atheroma. Circ Res. 1998b;83:1015–1026. - PubMed
-
- Aikawa M, Voglic SJ, Sugiyama S, Rabkin E, Taubman MB, Fallon JT, Libby P. Dietary lipid lowering reduces tissue factor expression in rabbit atheroma. Circulation. 1999;100:1215–1222. - PubMed
-
- Armstrong ML, Megan MB. Arterial fibrous proteins in cynomolgus monkeys after atherogenic and regression diets. Circ Res. 1975;36:256–261. - PubMed
-
- Belalcazar LM, Merched A, Carr B, Oka K, Chen KH, Pastore L, Beaudet A, Chan L. Long-term stable expression of human apolipoprotein A-I mediated by helper-dependent adenovirus gene transfer inhibits atherosclerosis progression and remodels atherosclerotic plaques in a mouse model of familial hypercholesterolemia. Circulation. 2003;107:2726–2732. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical