

Folate and cobalamin deficiencies and hyperhomocysteinemia in Bangladesh
- PMID: 15941889
- PMCID: PMC2204145
- DOI: 10.1093/ajcn/81.6.1372
Folate and cobalamin deficiencies and hyperhomocysteinemia in Bangladesh
Abstract
Background: Indian Asian men residing in the United Kingdom have a higher prevalence of hyperhomocysteinemia than do their European counterparts. This has been largely attributed to dietary deficiencies in cobalamin associated with vegetarianism among these Indian Asians.
Objective: We aimed to ascertain the prevalence of folate and cobalamin deficiencies and hyperhomocysteinemia in Bangladesh.
Design: Plasma concentrations of homocysteine, folate, and cobalamin and urinary concentrations of creatinine were assessed in 1650 adults in Bangladesh.
Results: The prevalence of hyperhomocysteinemia (men: >11.4 micromol/L; women: >10.4 micromol/L) was markedly (P < 0.0001) greater among men (63%; x +/- SD: 15.3 +/- 9.5 micromol/L) than among women (26%; 9.5 +/- 4.7 micromol/L). Folate was lower (9.8 +/- 6.5 and 12.3 +/- 7.6 nmol/L, respectively), whereas cobalamin was higher (281 +/- 115 and 256 +/- 118 pmol/L, respectively) (P < 0.0001 for both) among men than among women. Folate explained 15% and cobalamin explained 5% of the variation in homocysteine concentrations. For men, folate (P = 0.005) and cobalamin (P = 0.03) were positively correlated with urinary creatinine. Smoking (P < 0.0003) and betelnut use (P < 0.0002) were independent negative predictors of folate.
Conclusions: Bangladeshi men have a high prevalence of hyperhomocysteinemia, which is more closely associated with folate than with cobalamin, although other factors, eg, smoking and betelnut use, may also contribute to its cause. The positive correlations between urinary creatinine and plasma folate and cobalamin were unanticipated and could suggest that, in marginal nutrition, these vitamins may be limiting for creatine biosynthesis.
Figures
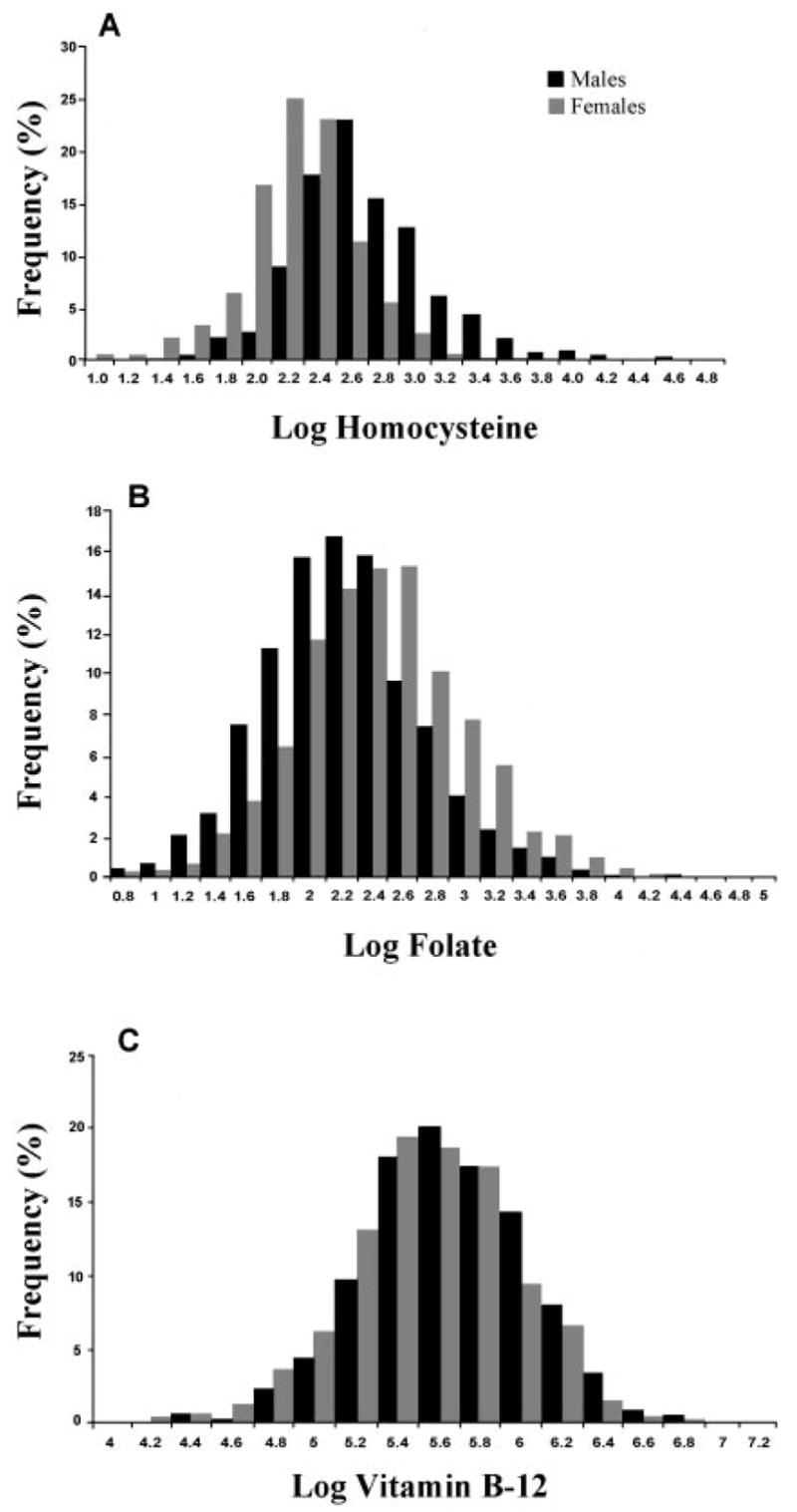
 ) and men (
) and men (
 ) for homocysteine (A; n = 676 M; n = 968 F), folate (B; n = 676 M; n = 972 F), and cobalamin (C; n = 676 M; n = 972 F). Homocysteine, folate, and cobalamin were skewed and were, therefore, log transformed.
) for homocysteine (A; n = 676 M; n = 968 F), folate (B; n = 676 M; n = 972 F), and cobalamin (C; n = 676 M; n = 972 F). Homocysteine, folate, and cobalamin were skewed and were, therefore, log transformed.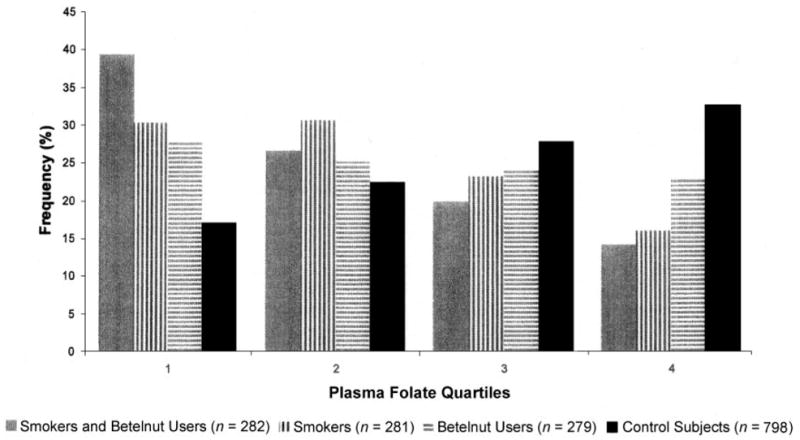
References
-
- Carmel R. Folate deficiency. In: Carmel R, Jacobsen DW, editors. Homocysteine in health and disease. Cambridge, United Kingdom: Cambridge University Press; 2001. pp. 271–88.
-
- Ubbink JB. What is a desirable homocysteine level? In: Carmel R, Jacobson CF, editors. Homocysteine in health and disease. Cambridge, United Kingdom: Cambridge University Press; 2001. pp. 485–90.
-
- Chambers JC, Obeid OA, Refsum H, et al. Plasma homocysteine concentrations and risk of coronary heart disease in UK Indian Asian and European men. Lancet. 2000;355:523–7. - PubMed
-
- Williams LJ, Mai CT, Edmonds LD, et al. Prevalence of spina bifida and anencephaly during the transition to mandatory folic acid fortification in the United States. Teratology. 2002;66:33–9. - PubMed
-
- Jacques PF, Selhub J, Bostom AG, Wilson PW, Rosenberg IH. The effect of folic acid fortification on plasma folate and total homocysteine concentrations. N Engl J Med. 1999;340:1449–54. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
