

Respiratory rehabilitation after acute exacerbation of COPD may reduce risk for readmission and mortality -- a systematic review
- PMID: 15943867
- PMCID: PMC1164434
- DOI: 10.1186/1465-9921-6-54
Respiratory rehabilitation after acute exacerbation of COPD may reduce risk for readmission and mortality -- a systematic review
Abstract
Background: Acute exacerbations of chronic obstructive pulmonary disease (COPD) represent a major burden for patients and health care systems. Respiratory rehabilitation may improve prognosis in these patients by addressing relevant risk factors for exacerbations such as low exercise capacity. To study whether respiratory rehabilitation after acute exacerbation improves prognosis and health status compared to usual care, we quantified its effects using meta-analyses.
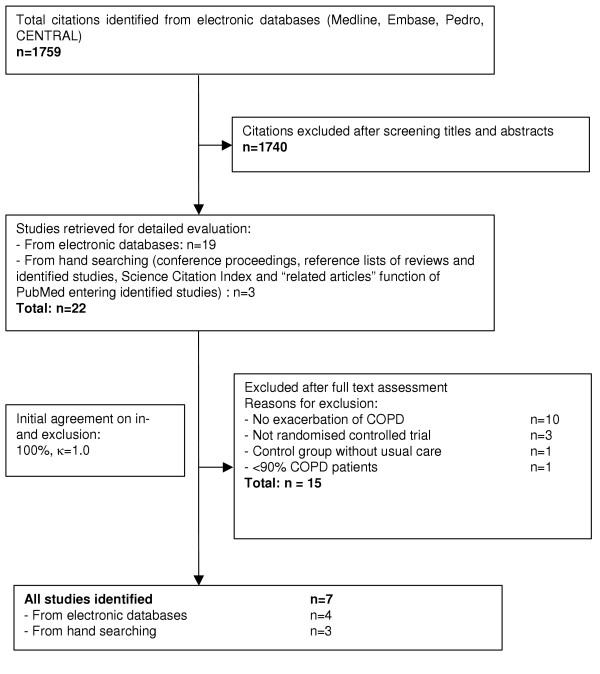
Methods: Systematic review of randomized controlled trials identified by searches in six electronic databases, contacts with experts, hand-searches of bibliographies of included studies and conference proceedings. We included randomized trials comparing the effect of respiratory rehabilitation and usual care on hospital admissions, health-related quality of life (HRQL), exercise capacity and mortality in COPD patients after acute exacerbation. Two reviewers independently selected relevant studies, extracted the data and evaluated the study quality. We pooled the results using fixed effects models where statistically significant heterogeneity (p < or = 0.1) was absent.
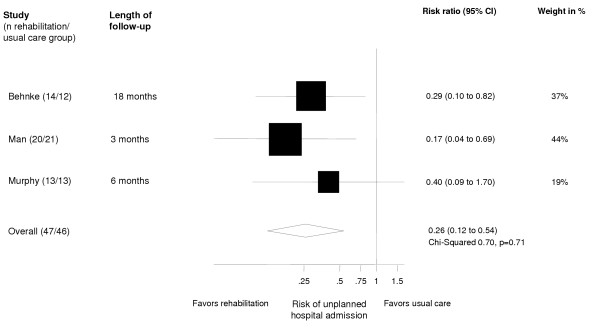
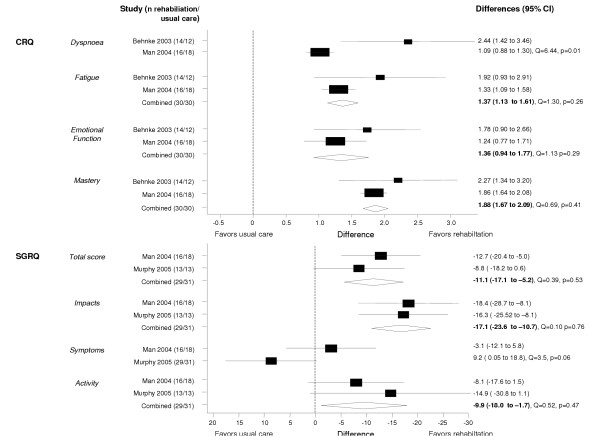
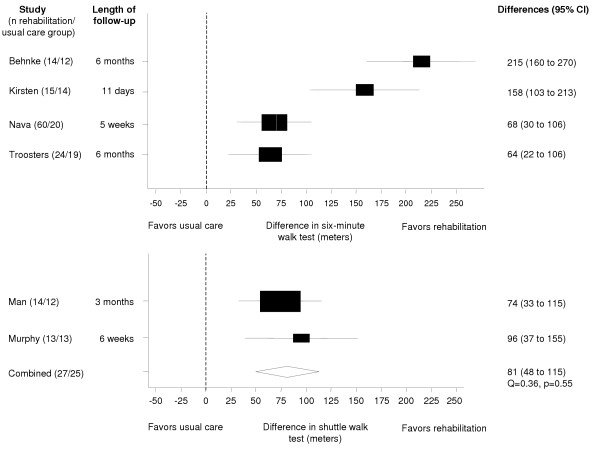
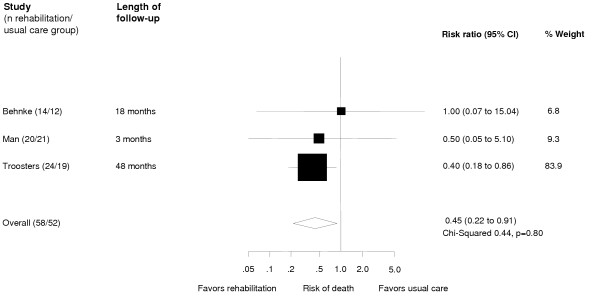
Results: We identified six trials including 230 patients. Respiratory rehabilitation reduced the risk for hospital admissions (pooled relative risk 0.26 [0.12-0.54]) and mortality (0.45 [0.22-0.91]). Weighted mean differences on the Chronic Respiratory Questionnaire were 1.37 (95% CI 1.13-1.61) for the fatigue domain, 1.36 (0.94-1.77) for emotional function and 1.88 (1.67-2.09) for mastery. Weighted mean differences for the St. Georges Respiratory Questionnaire total score, impacts and activities domains were -11.1 (95% CI -17.1 to -5.2), -17.1 (95% CI -23.6 to -10.7) and -9.9 (95% CI -18.0 to -1.7). In all trials, rehabilitation improved exercise capacity (64-215 meters in six-minute walk tests and weighted mean difference for shuttle walk test 81 meter, 95% CI 48-115).
Conclusion: Evidence from six trials suggests that respiratory rehabilitation is effective in COPD patients after acute exacerbation. Larger trials, however, are needed to further investigate the role of respiratory rehabilitation after acute exacerbation and its potential to reduce costs caused by COPD.
Figures
References
-
- Seemungal T, Donaldson G, Paul E, Bestall J, Jeffries D, Wedzicha JADW. Effect of Exacerbation on Quality of Life in Patients with Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 1998;157:1418–1422. - PubMed
-
- Connors AFJ, Dawson NV, Thomas C, Harrell FEJ, Desbiens N, Fulkerson WJ, Kussin P, Bellamy P, Goldman L, Knaus WA. Outcomes following acute exacerbation of severe chronic obstructive lung disease. The SUPPORT investigators (Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments) 1. Am J Respir Crit Care Med. 1996;154:959–967. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
