

Determinants of persistence in hypertensive patients treated with irbesartan: results of a postmarketing survey
- PMID: 15943871
- PMCID: PMC1166543
- DOI: 10.1186/1471-2261-5-13
Determinants of persistence in hypertensive patients treated with irbesartan: results of a postmarketing survey
Abstract
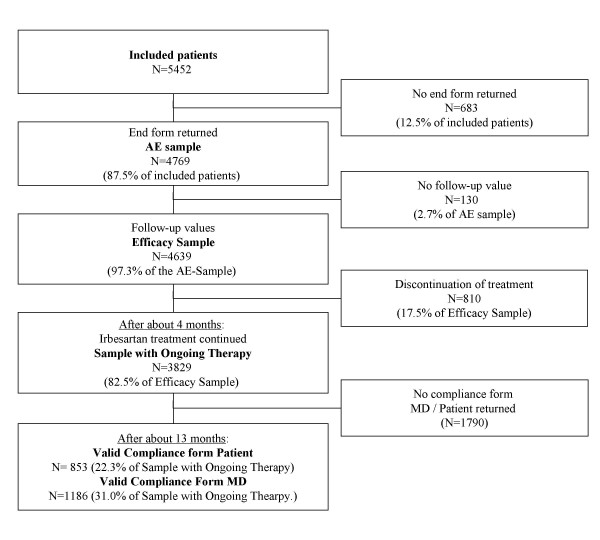
Background: Persistence is a key factor for long-term blood pressure control, which is of high prognostic importance for patients at increased cardiovascular risk. Here we present the results of a post-marketing survey including 4769 hypertensive patients treated with irbesartan in 886 general practices in Switzerland. The goal of this survey was to evaluate the tolerance and the blood pressure lowering effect of irbesartan as well as the factors affecting persistence in a large unselected population.
Methods: Prospective observational survey conducted in general practices in all regions of Switzerland. Previously untreated and uncontrolled pre-treated patients were started with a daily dose of 150 mg irbesartan and followed up to 6 months.
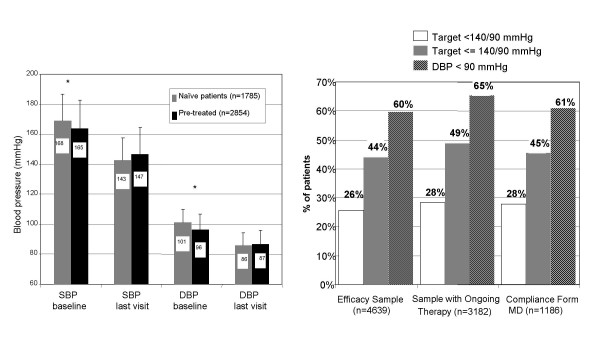
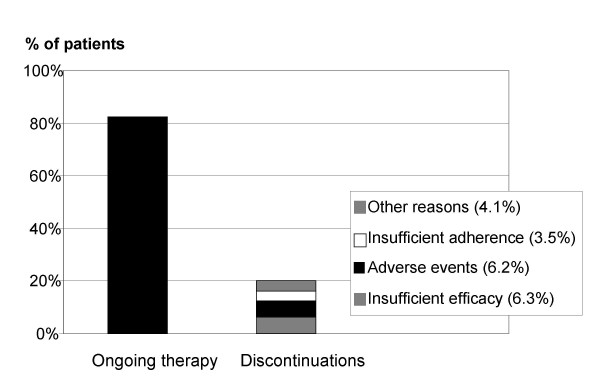
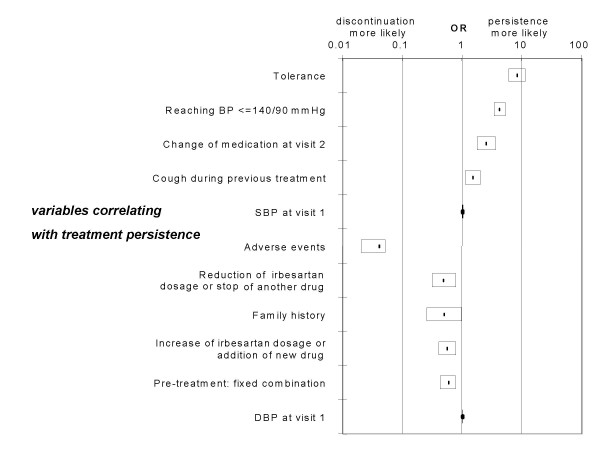
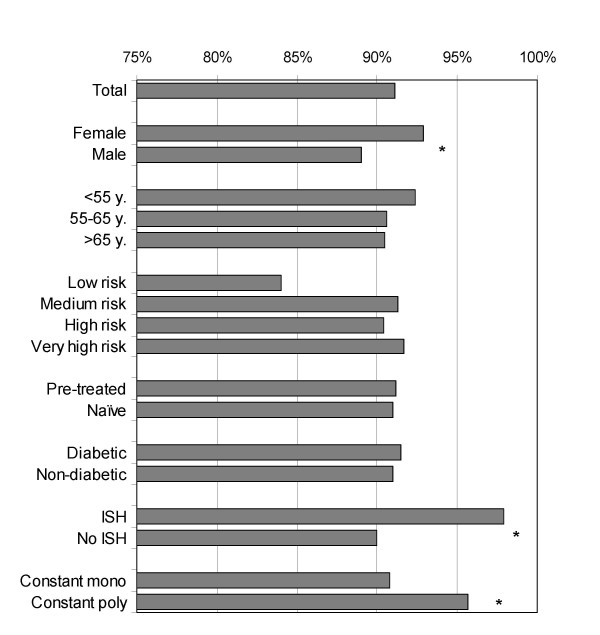
Results: After an observation time slightly exceeding 4 months, the average reduction in systolic and diastolic blood pressure was 20 (95% confidence interval (CI) -19.6 to -20.7 mmHg) and 12 mmHg (95% CI -11.4 to -12.1 mmHg), respectively. At this time, 26% of patients had a blood pressure < 140/90 mmHg and 60% had a diastolic blood pressure < 90 mmHg. The drug was well tolerated with an incidence of adverse events (dizziness, headaches,...) of 8.0%. In this survey more than 80% of patients were still on irbesartan at 4 month. The most important factors predictive of persistence were the tolerability profile and the ability to achieve a blood pressure target < or = 140/90 mmHg before visit 2. Patients who switched from a fixed combination treatment tended to discontinue irbesartan more often whereas those who abandoned the previous treatment because of cough (a class side effect of ACE-Inhibitors) were more persistent with irbesartan.
Conclusion: The results of this survey confirm that irbesartan is effective, well tolerated and well accepted by patients, as indicated by the good persistence. This post-marketing survey also emphasizes the importance of the tolerability profile and of achieving an early control of blood pressure as positive predictors of persistence.
Figures
Similar articles
-
Irbesartan for the treatment of hypertension in patients with the metabolic syndrome: a sub analysis of the Treat to Target post authorization survey. Prospective observational, two armed study in 14,200 patients.Cardiovasc Diabetol. 2007 Apr 3;6:12. doi: 10.1186/1475-2840-6-12. Cardiovasc Diabetol. 2007. PMID: 17407587 Free PMC article.
-
Effect of three months' treatment with irbesartan on blood and pulse pressure of hypertensive type 2 diabetic patients: open, observational study in 31,793 patients.Curr Med Res Opin. 2005 Sep;21(9):1433-40. doi: 10.1185/030079905X61811. Curr Med Res Opin. 2005. PMID: 16197662
-
BP goal achievement in patients with uncontrolled hypertension : results of the treat-to-target post-marketing survey with irbesartan.Clin Drug Investig. 2007;27(11):783-96. doi: 10.2165/00044011-200727110-00005. Clin Drug Investig. 2007. PMID: 17914897
-
Comprehensive overview: efficacy, tolerability, and cost-effectiveness of irbesartan.Vasc Health Risk Manag. 2013;9:575-92. doi: 10.2147/VHRM.S50831. Epub 2013 Oct 7. Vasc Health Risk Manag. 2013. PMID: 24124375 Free PMC article. Review.
-
AT1-receptor antagonism in hypertension: what has been learned with irbesartan?Expert Rev Cardiovasc Ther. 2003 May;1(1):23-33. doi: 10.1586/14779072.1.1.23. Expert Rev Cardiovasc Ther. 2003. PMID: 15030294 Review.
Cited by
-
Effectiveness and tolerability of a trandolapril-based antihypertensive treatment regimen over 12 months in actual clinical care across Canada.Clin Drug Investig. 2013 Aug;33(8):535-43. doi: 10.1007/s40261-013-0092-y. Clin Drug Investig. 2013. PMID: 23784370
-
Safety and tolerability of the direct renin inhibitor aliskiren in combination with angiotensin receptor blockers and thiazide diuretics: a pooled analysis of clinical experience of 12,942 patients.J Clin Hypertens (Greenwich). 2011 Jul;13(7):506-16. doi: 10.1111/j.1751-7176.2011.00438.x. Epub 2011 Mar 18. J Clin Hypertens (Greenwich). 2011. PMID: 21762364 Free PMC article.
-
Safety and tolerability of the direct renin inhibitor aliskiren: a pooled analysis of clinical experience in more than 12,000 patients with hypertension.J Clin Hypertens (Greenwich). 2010 Oct;12(10):765-75. doi: 10.1111/j.1751-7176.2010.00352.x. J Clin Hypertens (Greenwich). 2010. PMID: 21029339 Free PMC article.
-
Patient adherence and the choice of antihypertensive drugs: focus on lercanidipine.Vasc Health Risk Manag. 2008;4(6):1159-66. doi: 10.2147/vhrm.s3510. Vasc Health Risk Manag. 2008. PMID: 19337529 Free PMC article. Review.
-
Effects of initial antihypertensive drug class on patient persistence and compliance in a usual-care setting in the United States.J Clin Hypertens (Greenwich). 2007 Sep;9(9):692-700. doi: 10.1111/j.1524-6175.2007.07194.x. J Clin Hypertens (Greenwich). 2007. PMID: 17786070 Free PMC article.
References
-
- Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJ, Michelson EL, Olofsson B, Ostergren J, Yusuf S, Pocock S. CHARM Investigators and Committees. Effects of candesartan on mortality and morbidity in patients with chronic heart failure: the CHARM-Overall programme. Lancet. 2003;362:759–66. doi: 10.1016/S0140-6736(03)14282-1. - DOI - PubMed
-
- Lindholm LH, Ibsen H, Dahlof B, Devereux RB, Beevers G, de Faire U, Fyhrquist F, Julius S, Kjeldsen SE, Kristiansson K, Lederballe-Pedersen O, Nieminen MS, Omvik P, Oparil S, Wedel H, Aurup P, Edelman J, Snapinn S, LIFE Study Group Cardiovascular morbidity and mortality in patients with diabetes in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet. 2002;359:1004–10. doi: 10.1016/S0140-6736(02)08090-X. - DOI - PubMed
-
- Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB, Ritz E, Atkins RC, Rohde R, Raz I. Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851–60. doi: 10.1056/NEJMoa011303. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
