

Reinfection and mixed infection cause changing Mycobacterium tuberculosis drug-resistance patterns
- PMID: 15947286
- PMCID: PMC2718533
- DOI: 10.1164/rccm.200503-449OC
Reinfection and mixed infection cause changing Mycobacterium tuberculosis drug-resistance patterns
Abstract
Rationale: Multiple infections with different strains of Mycobacterium tuberculosis may occur in settings where the infection pressure is high. The relevance of mixed infections for the patient, clinician, and control program remains unclear.
Objectives: This study aimed to describe reinfection and mixed infection as underlying mechanisms of changing drug-susceptibility patterns in serial sputum cultures.
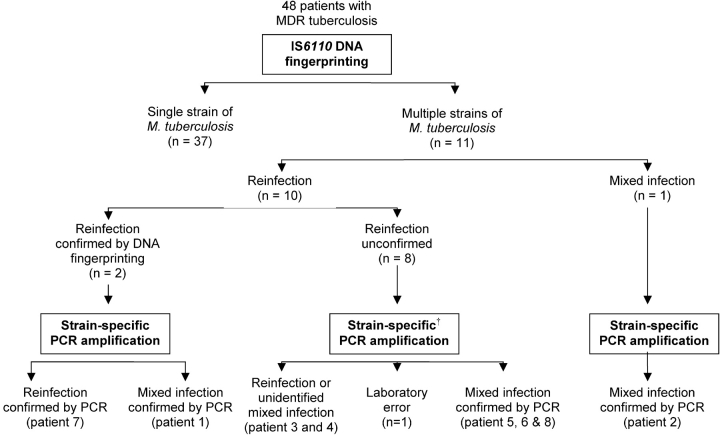
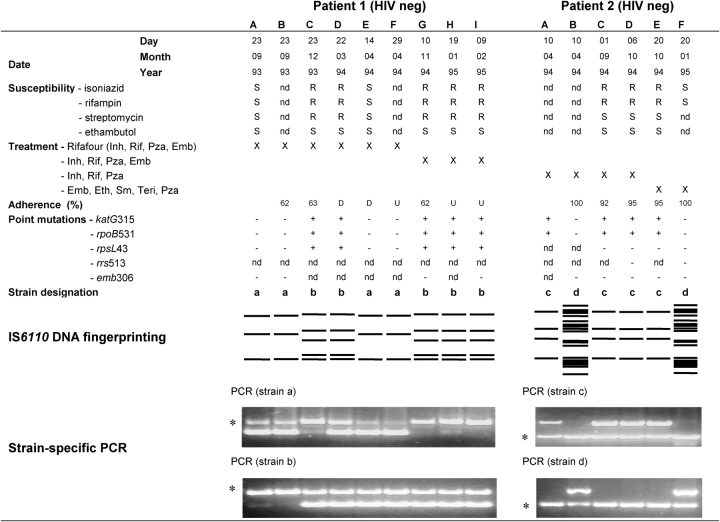
Methods: Serial M. tuberculosis sputum cultures from patients diagnosed with multi-drug-resistant (MDR) tuberculosis were evaluated by phenotypic drug-susceptibility testing and mutation detection methods. Genotypic analysis was done by IS6110 DNA fingerprinting and a novel strain-specific polymerase chain reaction amplification method.
Measurements and main results: DNA fingerprinting analysis of serial sputum cultures from 48 patients with MDR tuberculosis attributed 10 cases to reinfection and 1 case to mixed infection. In contrast, strain-specific polymerase chain reaction amplification analysis in 9 of the 11 cases demonstrated mixed infection in 5 cases, reinfection in 3 cases, and laboratory contamination in 1 case. Analysis of clinical data suggests that first-line therapy can select for a resistant subpopulation, whereas poor adherence or second-line therapy resulted in the reemergence of the drug-susceptible subpopulations.
Conclusions: We have shown that, in some patients with MDR tuberculosis, mixed infection may be responsible for observations attributed to reinfection by DNA fingerprinting. We conclude that treatment and adherence determines which strain is dominant. We hypothesize that treatment with second-line drugs may lead to reemergence of the drug-susceptible strain in patients with mixed infection.
Figures
Comment in
-
Polyclonal tuberculosis and the emergence of drug resistance.Am J Respir Crit Care Med. 2005 Sep 1;172(5):521-2. doi: 10.1164/rccm.2506008. Am J Respir Crit Care Med. 2005. PMID: 16120715 No abstract available.
References
-
- Stead WW. Pathogenesis of a first episode of chronic pulmonary tuberculosis in man: recrudescence of residuals of the primary infection or exogenous reinfection? Am Rev Respir Dis 1967;95:729–745. - PubMed
-
- van Rie A, Warren R, Richardson M, Victor TC, Gie RP, Enarson DA, Beyers N, van Helden PD. Exogenous reinfection as a cause of recurrent tuberculosis after curative treatment. N Engl J Med 1999;341:1174–1179. - PubMed
-
- Small PM, Shafer RW, Hopewell PC, Singh SP, Murphy MJ, Desmond E, Sierra MF, Schoolnik GK. Exogenous reinfection with multidrug-resistant Mycobacterium tuberculosis in patients with advanced HIV infection. N Engl J Med 1993;328:1137–1144. - PubMed
-
- Caminero JA, Pena MJ, Campos-Herrero MI, Rodriguez JC, Afonso O, Martin C, Pavon JM, Torres MJ, Burgos M, Cabrera P, et al. Exogenous reinfection with tuberculosis on a European island with a moderate incidence of disease. Am J Respir Crit Care Med 2001;163:717–720. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
